

Unknown Side-Effects of Prilosec (and PPIs): From Hearing Loss to Stomach Cancer.
The risks your doctor does NOT know about when he's "treating" your heartburn with proton-pump inhibitors.

I’ve been researching heartburn, reflux and all its consequences for a number of years. The most important driver for this research is that there are so many people around me who suffer from chronic or acute bouts of heartburn.
I know many people taking drugs like Prilosec (brand name of omeprazole) for extended periods of time, because it provides variable symptomatic relief. But, without ever really addressing the underlying cause.
If you’ve read my past work, you will know that heartburn doesn’t have a single cause. Sure, there are common causes…but, it is highly variable.
Heartburn/reflux can be caused by disc herniations, thyroid disease, diaphragm dysfunction and even low stomach acid.

That’s right. Low stomach acid. Not high stomach acid, as most doctors will have you believe before they whip out their pad to prescribe a proton-pump inhibitor.
I’ve had success curing heartburn and its associated problems in many people. Recently, one of my readers underwent an experimental red light protocol that I developed from the research uncovered in the last couple of years. Pr
For the first time in years, she has “had an unprecedented 3 weeks, without any issues at all.”

At this point, I’m confident that the framework I’ve developed for understanding and treating heartburn is superior to most others.
But, this article isn’t about how to treat heartburn.
This article is about what to avoid!
The Standard Model
Heartburn is such a common problem that most people know exactly the steps that follow.
You go to the doctor, describe typical (or atypical) symptoms of gastroesophageal reflux, and he makes a couple of dietary recommendations, but ultimately prescribes a proton-pump inhibitor (such as Nexium or Prilosec).
You take this drug, experience variable symptomatic relief…and move on with your day.
There’s hardly any discussion of side-effects, short or long-term. Mostly because the doctor isn’t aware of them.
As far as he is concerned, heartburn is caused by too much acid. So suppressing acid secretion with PPIs is the conclusion.
It’s considered so benign that you can go to Costco and purchase large quantities of this drug without a prescription.
If you are reading this, you already know there’s more to this story…
In this article we will review:
Why doctors recommend proton-pump inhibitors for treatment of heartburn
Why this is misguided and ill-advised
The various mechanisms by which PPIs can exert harmful effects on your body
Studies exploring their effects on the stomach
New studies observing effects on several other body systems including the psyche, kidneys, pancreas, hearing (cochlea), and even immune system.
Why Recommend PPIs?
During medical training doctors are taught that heartburn is caused by ‘too much stomach acid.’ Which isn’t entirely accurate.
A more appropriate way of phrasing this is:
The sensation of heartburn is a result of stomach acid moving backwards up into the esophagus and irritating the surrounding structures.
Notice, I didn’t say anything about “too much stomach acid.” Because more often than not, the sensation of ‘heartburn’ is not caused by excess acid. Instead, it is caused by the inappropriate movement of acid.
More importantly, the inappropriate movement of acid happens when there is less than normal quantity of acid in stomach.
In addition to the mechanisms outline in the Root Cause article above, just look at the overlapping symptoms in people experiencing heartburn and those with low stomach acid (achlorhydria):

What’s Wrong With PPIs?
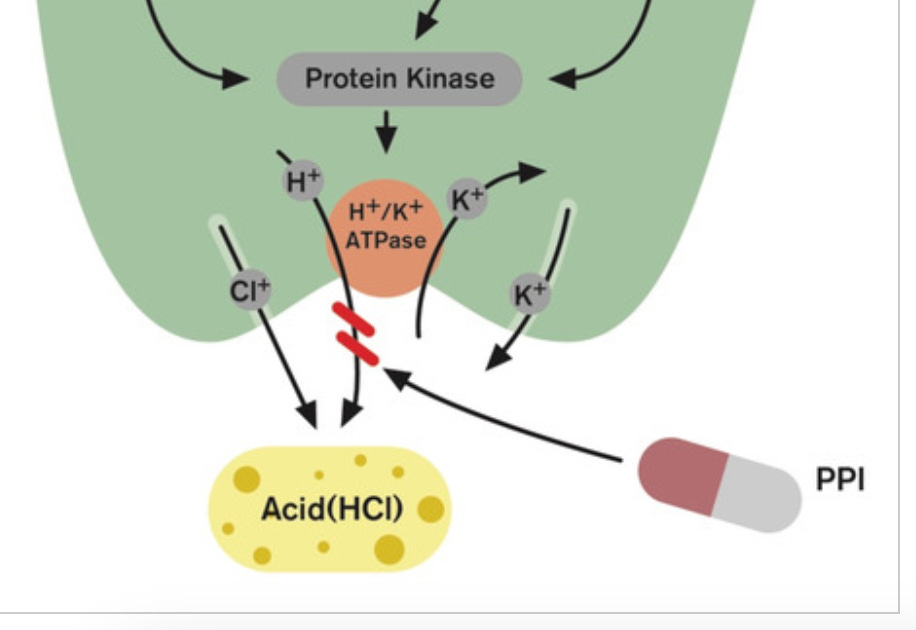
As the name suggests, PPIs inhibit the action of membrane pumps which shuttle protons in and out of cells. In the stomach, this targets the hydrogen/potassium pump (H+/K+ ATPase). Thereby reducing the secretion of acid into the stomach.
To illustrate the first problem with PPIs, a friend of mine remarked:
Proton-pump inhibitor?
We don’t really use proton pumps for anything important, do we?
Of course, he was joking.
Proton pumps are one of the most ubiquitous membrane proteins in all of biology, in part because protons (AKA Hydrogen ions H+) are the most common ion in nature.
Hydrogen ions are shuttled in and out of cells throughout the body, with or without the exchange of other ions.
For instance, your local certified drug-dealer may claim that Omeprazole is specific to H+/K+ pumps in the stomach. And, he’d be wrong.
Not only does omeprazole affect H+/K+ pumps in other parts of the body, but new evidence demonstrates its impact on intracellular H+ ATPase channels. Meaning, pumps inside of the cell used for cellular function and communication are also inhibited by this “specific” PPI.
Secondly, even if the effect of PPIs was specific to the stomach, why would you consider interfering with the stomach’s natural function for an extended period of time?
You are asking for trouble.
What sort of trouble? Well, let’s dig in.
Risks of Extended PPI Use
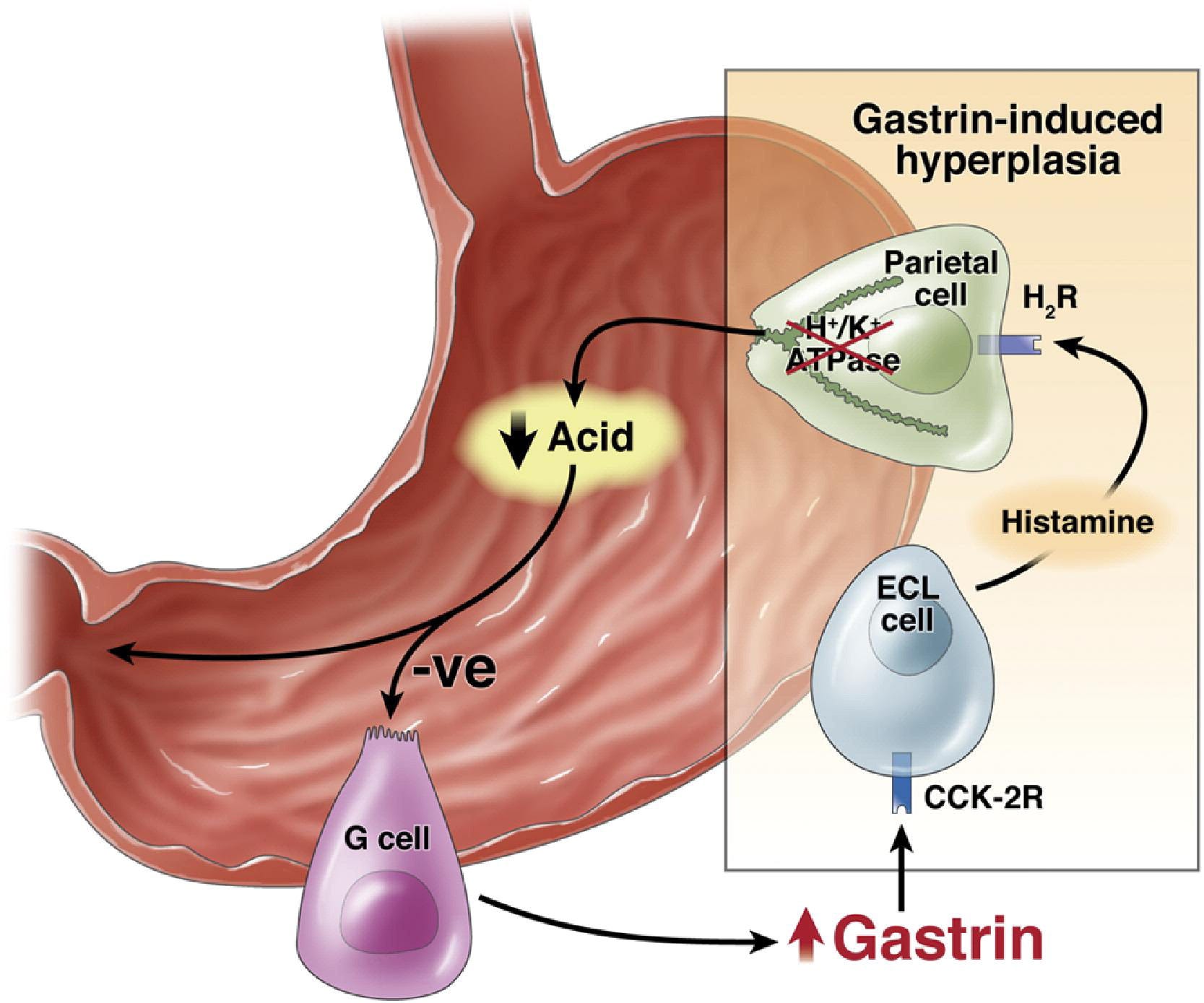
The above image illustrates the feedback mechanism between different cells of the stomach including the role of PPIs in inhibiting acid release from Parietal cells .
The inhibition of acid release stimulates G cells to release Gastrin.
Gastrin, in turn, acts on ECL (enterochromaffin-like cells) to release more Histamine. Because the PPI prevents the feedback mechanism that stops the release of gastrin, you get runaway over-activation of both G cells and ECL cells.
This comes with many consequences we need to consider:
These cells get larger (hyperplastic) and grow in number from overstimulation.
ECL cells release more than just histamine; it also produces and secretes serotonin.
I believe its role in serotonin dysregulation is a main driver for the newly observed relationship between PPI use and depression - in both the elderly and children:
ECL cells also produce and release melatonin, which co-incidentally may be the main driver of symptom relief in people who take PPIs for heartburn
melatonin is somewhat of a miracle for reflux and its complications.

Are there any other effects of this overstimulation?
Oh, you bet. Buckle-up.
Changes in Stomach Lining
High levels of gastrin don’t just stimulate release of other signaling molecules. Like any hormone that positively stimulates a cell, it also leads to cell growth and replication. Thus, PPI use leads to a combination of trophic (growth-related) effects on the cells of the stomach.
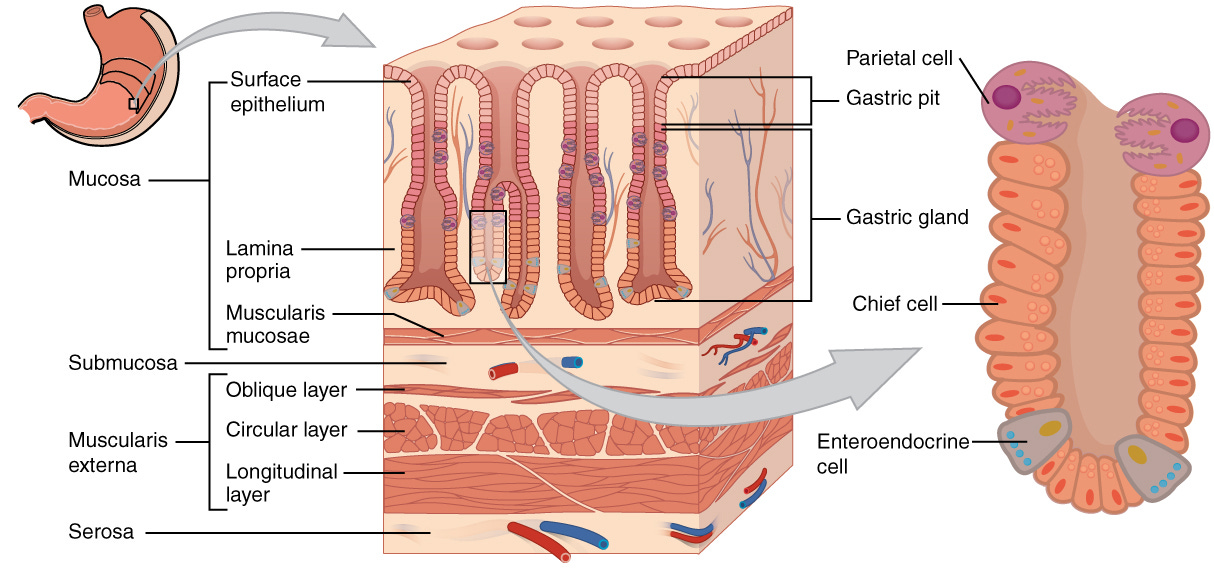
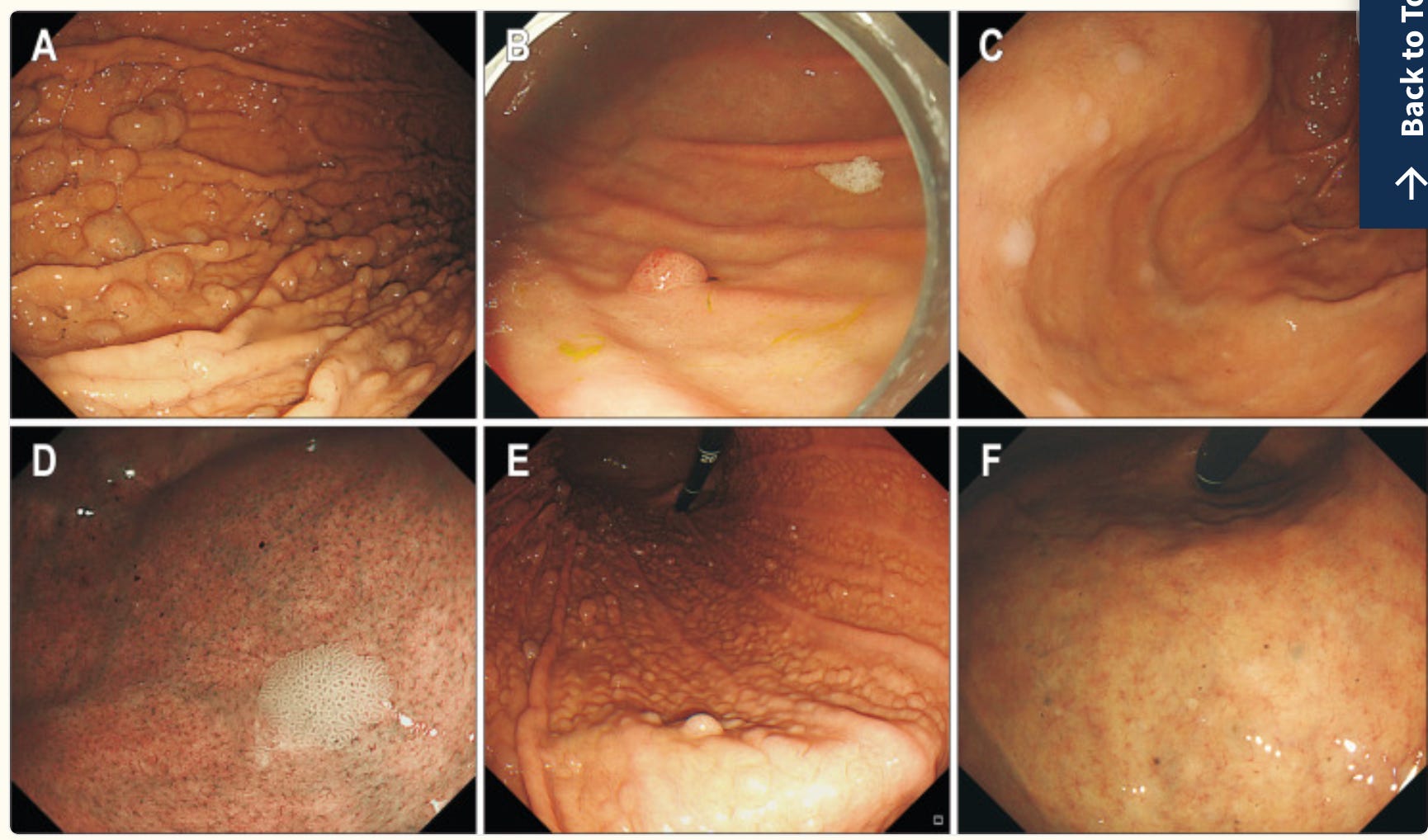
First, it has been observed that parietal cells swell. As you can see in the image, if these cells swell, it leads to protrusion and obstruction of the pits along the inner lining of stomach.
These lead to obstructive and cystic changes along the lining. The consequences of which are many and varied including: formation of polyps, atrophy of the stomach lining, necrosis/death of the cells along these pits which manifest as tiny black dots during endoscopic examination, and even cancer.
Yes, I said cancer.
One of the things that’s been observed since the advent of PPIs (in the late 1970s) is the change in diagnosis of cancers of neuroendocrine origin. Stay with me here.
Enterochromaffin cells are of neuro-endocrine origin. Thus, anything that disrupts the function of neuro-endocrine cells (such as the effect of PPIs on ECL cells), will ultimately result in growth of neuroendocrine tumors like gastric carcinoid, amongst other forms of carcinoid tumors.
Dr. McCarthy observes an interesting relationship in the period after the introduction of PPIs. The rates of carcinoid tumors has exploded. Overall, a 7-fold increase across all carcinoid tumors.
The highest increase was in stomach carcinoid tumors; about 15-fold increase.
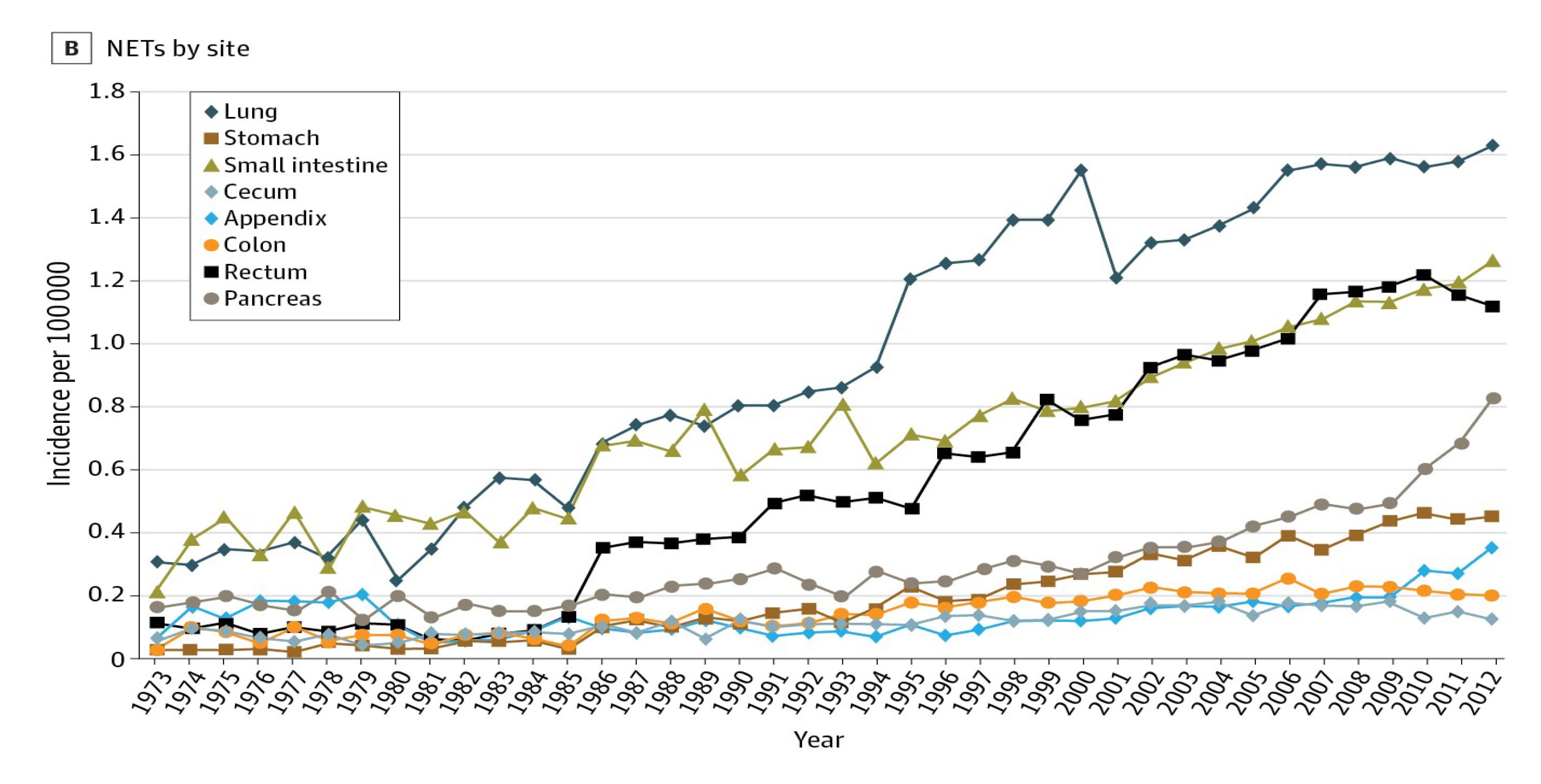
It isn’t just neuroendocrine tumors of the stomach which are seeing a rise with chronic use of PPIs. The data on this is shocking. Here are a couple of examples you can peruse:
More than twofold increase risk of gastric cancer
Approximately 1.75-fold increase risk of pancreatic cancer

Hearing Loss
Remember when I said that proton-pumps are ubiquitous and exist everywhere in the body?
You’ll never guess where the exact proton-pump also exists?
In the cochlea - the apparatus our brain uses to hear.
And so, one has to wonder what happens when our bloodstream is constantly moving a drug with the sole purpose of inhibiting this proton pump.
Turns out, you get chronic loss of hearing.
One study from South Korea demonstrated that even using PPIs for as little as 30 days straight resulted in higher odds of hearing impairment. Whether you used it for less than or more than a year, the odds were comparable (1.65x vs 1.52x).
Interestingly, the gastric proton pump found in the cochlea has also been found in the choroid plexus (cells inside the ventricles of the brain) in rat brains. The impact of cerebrospinal fluid may also impart an effect on the brain as well as the cranial nerves which serve hearing and other functions.
Impact on the Immune System and Beyond
Remember when I said that Omeprazole also inhibits Vacuolar Proton pumps?
One of these pumps is called V-ATPase. This pump is present in sub-cellular organelles of osteoclasts (bone cells) and renal tubular epithelial cells (kidney cells), for instance.
We will return to bones and kidneys in a moment.
Besides pumping protons, V-ATPase is also involved in differentiation of immune T-cells (specifically CD4+ T-cells). It seems to have a particular impact on T-helper 1 and T-helper 17 proliferation.
One study analyzing the growth of these immune cells finds that Omeprazole leads to suppression of CD4+ T-cell growth, possibly accounting for increased susceptibility to infection. Secondly, they observe that the constellation of T-cell effects is one that favors a picture similar to autoimmune disease.
Probably related to effects on the same V-ATPase, there has been emerging observation that chronic use of PPIs also impacts kidney function.
Some studies have observed new-onset kidney dysfunction, and others have observed worsening chronic kidney disease in people taking PPIs.
Then, there’s the impact on bones and the risk of osteoporosis related fractures:
I Think You Get it.
The story of PPIs reminds me of the story of statins (a cholesterol lowering drug).
These two drugs aim to solve a very common problem, but do so in the most non-specific way imaginable.
They target a set of proteins which are so ubiquitous, that their side-effects far outweigh any potential benefit they may provide.
In the case of PPIs, we are targeting enzymes which move hydrogen ions into and out of cells. A very broad action.
Similarly, statins inhibit the production of mevalonate, which is a precursor to hundreds if not thousands of cholesterol-derived molecules that are integral to the function of the body.

If you found this article eye-opening, consider sharing it with others.
Also, stay tuned for a complete guide on how to treat, reverse, and prevent heartburn.
I managed to heal most of my problems by using apple cider vinegar and herbal bitters. But I still felt like things weren't completely healed. My clinic recommended cabbage juice. It's a Korean product with a bit of Manuka honey. You can feel the inflammation go down in the esophagus.
Wonderful review. Also learn some new things about the side effects of taking these drugs. Thank you for that