

What Alchemy, Gold, and Curly Hair Have to Do With Your Heart
Tracing the hidden role of sulfur through sunlight, cholesterol, and disease.

On the journey of uncovering our lost medical traditions, I found myself tangentially exploring the history of alchemy.
The standard alchemical conundrum is how to make gold from other elements, such as lead. Unfortunately for us, alchemical texts are written in relatively impenetrable prose and lingo.
But one thing that stuck out to me was the relationship described with the Sun. Almost as if the Sun is an integral component of this recipe to make gold.
According to a quick search, it seems that the presence of sulfur deep in the earth allows for gold to be dissolved and transported to the crust as gold ore deposits, rather than be dispersed through magma and hydrothermal fluids below.
Now, I could be way off base here, but this lead me to think of the Sun in many ways. Sulfur and sulfation seems to be one of the common threads throughout biology, as it seems to be with mineral deposits.
Sulfur and Sulfation

Sulfur is the 5th most common element on earth. It is essential to all life in more ways than one. It plays a role in structural, communication, metabolic, and endocrine functions.
Its properties lend it to form flexible, reversible, and redox-sensitive bonds. The importance of sulfur can be seen at many levels of organization within living matter.
You can think of life as consisting of carbon (which gives structure), nitrogen (which forms amino acids), and sulfur which gives life the ability to respond to its environment and needs.
For instance, the amino acids cysteine and methionine must contain sulfur. The “-thiol” groups indicate the presence of sulfur. But it’s not just these amino acids.
Glutathione (GSH), which is implicated in diverse anti-oxidative processes including liver capacity to process toxins, also has a critical sulfur group.
Coenzyme A, which is important for metabolism, especially of fatty acids, must contain sulfur. Additional it is important in production of ketones and steroids.
Sulfur can form disulfide bonds which stabilize proteins, and lend itself to the structural importance of sulfur. The disulfide bond allows proteins to fold, unfold, refold and undergo redox-related changes to its conformation.
Sulfation is the process of attaching a sulfate group (SO4) to a molecule, and it is catalyzed by enzymes in the sulfotransferase (SULT) family.
It’s a major pathway by which the body regulates hormones, shapes structure of tissue, maintain extracellular integrity, and detox substances.
For example, sulfation is involved with deactivation of estrogen or dopamine. It activates thyroid hormone from T4 to T3 via recycling. It modulates neurotransmitters and catecholamines. It also plays a role in bile acids.
Skin, Hair and Vitamin D
Hair (amongst other structures) is formed by keratin, with cysteine as a major amino acid constituent of the protein that makes up hair. If you recall, cysteine has a sulfur group.
It is the oxidation of these cysteine residues which catalyzes the di-sulfide bridge that forms between strands/loops of hair to give it structure, strength and shape. This oxidation occurs most naturally by sunlight, likely facilitated by UVB.
Thus it is the energy of the Sun which not only leads to proliferation of hair follicles (via Infrared/UV combination), but also to the shape and strengthening of the hair by disulfide bridges.
The degree to which the hair can have these properties depends on temperamental differences between individuals. For example, sulfur is thought of as a hot/heating/metabolically active constituent of our bodies.
People with hot temperaments (e.g. choleric) may indeed have a higher sulfur load. This can manifest in the presence of more cysteine residues in hair.

So, if you are of a hot and dry temperament, the combination of the cysteine residues and appropriate light exposure can lead to curly hair. Which is precisely what we observe in the stereotype of this temperament. And, is also expected in people with more sulfur bridges within their hair.
More cysteine → more bridges → more curls
The relationship between Sun and Sulfur don’t end there.
For example, it is well known that naturally produced vitamin D requires sunlight. But, people are under the impression that by simply taking a vitamin D supplement, they can reap all the benefits of this crucial vitamin.
This is not true.
The Sun and UVB enact two parallel pathways which ultimately lead to the production of biologically active and useful Vitamin D.
Our skin has a very large store of cholesterol sulfate, and sulfates in other conjugated forms. When these stores are hit by UVB, the target is oxidized, which then releases sulfate radicals. These radicals stabilize somewhat by formation of SO4 (sulfate) ions.
The other role of UVB is in the activation of Vitamin D production. UVB light converts 7-dehydrocholesterol to pre-vitamin D3. This unstable form then rearranges to Vitamin D3, which then becomes sulfated by that which was liberated above.
Together, these reactions form the original and physiologically potent form of Vitamin D3. Without the Sun, this is not possible.
Sulfated Vitamin D3 is unique in that it is able to enter the bloodstream and circulate freely. There is no need for carrier proteins or structures, such as LDL cholesterol particles. Unsulfated vitamin D3 needs these carriers.
Furthermore, sulfated Vitamin D3 is also more stable and can act as a reservoir of vitamin D3, when needed by the body.
Interestingly, this leads to a reinforcing positive feedback loop:
Vitamin D boosts our bodies sulfation capacity as 1,25-D3 upregulates the activity of
Sterol (cholesterol derived) sulfation
GAG (glycosaminoglycans) sulfation
detox by sulfotransferase enzymes
Even with normal blood levels of vitamin D (as reported in lab tests), without sulfation the expected beneficial effects of vitamin D are limited.
I believe this is one reason why we see conflicting data when trying to observe relationships between sunlight exposure and presence or absence of certain diseases. Because often times, when researchers are looking to gauge a participants sunlight exposure, they resort to blood Vitamin D levels.
However, many people take oral vitamin D…so even if their tests show higher levels…the effects of this vitamin D is limited, and the benefit isn’t appreciated.
This actually limits our understanding and appreciation of the role of vitamin D in many disease processes. One of which may be the confounding data on brain aneurysms:

Vitamin D, Cholesterol and Heart Disease
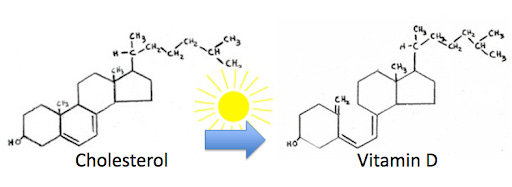
As the image above clarifies, the relationship between cholesterol and vitamin D is tight. In fact, the only difference is that in the presence of UV light, that single-bond in the bottom ring structure is broken.
Putting the nature of blood, blood vessels, and blow flow aside…you can start to see how the relationship between Sun, circulation and cholesterol is more complex than “cholesterol = bad.”

For starters, it’s important to know that just like sulfated vitamin D there is a difference between free cholesterol and sulfated cholesterol (or esterified cholesterol sulfate). As you may imagine, the same class of enzymes which sulfate other proteins and compounds also sulfated cholesterol.
Moreover, cholesterol sulfate is synthesized in the skin upon exposure to sunlight. In fact, it happens in similar locations and pathways by which vitamin D is formed by sunlight exposure.
Skin cells (keratinocytes) express SULT2B1b, the sterol-related sulfotransferase. Similar to vitamin D, the UV triggers the formation of sulfate radicals, and this radical is then attached to cholesterol.
Free (unsulfated or unesterified) cholesterol is an interesting topic. We are finding that atherosclerotic plaque are relatively rich in free cholesterol.
One reason that may be the case is that free cholesterol crystalizes. When the amount of free cholesterol in our body (and tissues/organs) gets too high, such that the process of esterification or transport is overwhelmed, these crystals mark the phase transition of fluid cholesterol to solid crystalline cholesterol.

Once they are formed, these crystals can accumulate in the subendothelial space and become the nidus of atheroma/plaque formation. These cholesterol crystals themselves are thought to be pro-inflammatory.
Thus, simply the presence of this form of cholesterol can have a feedback mechanism by which plaque worsens and eventually ruptures.
This is the best case argument in favor of the lipid hypothesis that simply high blood lipids are the causative agents of heart disease. As you can tell by the information above, this is obviously not the root cause. It is but one bystander process by which metabolic dysregulation leads to atherosclerosis.
For example, simply intake of oral vitamin D can lead to upregulation of lipoprotein particles (such as HDL or LDL) to carry this unsulfated vitamin and other unsulfated cholesterols in the bloodstream. These then deposit their payload into areas of high endothelial stress (which is independent of the presence cholesterol), and start the formation of atheromas or atherosclerotic plaques.
Signs of Low Sulfation Capacity
From a medical perspective “sulfur deficiency” isn’t really a thing. Because the amino acids which carry sulfur are abundant, it isn’t a diagnosis we tend to be concerned about.
However, that doesn’t mean that our metabolic pathways which depend on the presence of sulfated proteins do not become insufficient to deal with the needs and stresses of our daily lives.
Generally speaking, highly processed/refined foods are low in sulfur containing amino acids.
To complement the sulfur intake aspect, there is also the demand on sulfur and impairment of sulfur recycling.
Modern developed and industrial life tends to expend sulfation capacity. Whether it’s from environmental toxins, inflammatory stress, high estrogen load, or over-the-counter tylenol.
Furthermore, the recycling of sulfate requires:
oxygen-dependent metabolism
functional mitochondria
robust supply of glycine
Glycine is crucial in making/recycling Glutathione (GSH).
To assess if you are deficient in sulfation capacity there are lab tests you can perform (including GSH, homocysteine, and taurine levels).
However, a functional assessment may also be used:
Dry and fragile skin
Cracking along the heels
weak nails
thin hair
poor wound healing
joint stiffness
tendonitis/tendonopathy
Food irritability
Intolerance to tylenol
Mood lability
Poor stress tolerang
Estrogen dominance
Correcting the Deficiency
SUNLIGHT and foods rich in sulfur.
Sulfur Rich Foods:
Organ meat
eggs
Garlic and onions
Seafood
Wonderful summary and you got me thinking. I wonder if DMSO mechanism is related to the folding repair of proteins that its sulfur has. Also as a oncology pharmacist it is commonly observed that folks who undergo certain chemotherapies and lose their straight hair often grow it back curly. Sulfur maybe involved in that phenomenon?
I read the article twice. I don’t have any of the functional symptoms of sulfur deficiency so hopefully I’m ok. I upped my sulfur intake several years ago. I eat a clove of fresh garlic at least weekly, as well as broccoli sprouts, eggs, dimethylsulfoxide, and black garlic 3-7x a week.
For glycine I drink homemade bone broth. And I also take 1-2 teaspoons of powdered glycine daily. Sun exposure always seems to be a master lever for health.
Note- If company is coming I skip the garlic for a few days prior. 😁
Thanks for giving us actionable steps to correct and improve upon the deficiency issue. I do supplement D3 along with cofactors but try to get as much sun as I can. There is so much more for me to learn about D3.