

Is High Blood Pressure a Disease?
The entire framework of how we diagnose and treat blood pressure is built on a category error.
Part I: The Wrong Framework
There are two questions that every patient asks themselves as they walk into a doctor’s office.
What do I have?
What do I need to fix it?
Unfortunately, these are the wrong questions.
It’s not because patients are unsophisticated. It is because medicine has spent decades teaching people (including doctors) to ask them. The entire architecture of modern healthcare (diagnostic codes, treatment algorithms, and pharmaceuticals) is built on this framework. Several of the core clinical reference manuals (e.g. Merck Manual) are based on this framing.. That is not a coincidence. It’s an entire profession encoded in industry pairings.
The framework goes like this. Your body has malfunctioned. Name the malfunction. Correct the malfunction. Move on.
The problem is that the body doesn’t malfunction.
It responds. Every symptom, every sign, every number your doctor circles in red is the body’s attempt to compensate for something that came before. It is not broken. It is communicating.
The body is trying to tell you something.
Which begs the question…are you listening?
This question asks you to adopt a different position. On in which you try to understand, to reflect, to hear what the body is telling you. Instead of you telling the body it is malfunctioning and the doctor has just the prescription it needs.
Once you lock in on that…the solution follows naturally.
There is no better example of this than blood pressure.
Because it is the most aggressively treated, the most casually diagnosed, and the most misunderstood. It demonstrates the pipeline I described above perfectly.
Number → Label → Prescription
Without taking a moment to understand what the body is telling us.
And it is trying to tell us something.
I’m going to use the example of my mother’s insanely high blood pressure over the holidays to illustrate this guide, but if you want to read the dedicated article about the experience/process of getting her blood pressure as low as its ever been without medications - here it is:

The point is that she didn’t have hypertension. Her blood pressure was dysregulated.
Those are not the same statement. The first ends at a prescription.
The second begins with a question: who is she, and why is her body working this hard?
Part II: What Blood Actually Is
Most people think of blood as a delivery service. It carries oxygen to your tissues, picks up carbon dioxide, and cycles back. Red blood cells are the vehicles. The heart is the pump. Simple.
This picture is wrong.
Start with water. Blood is mostly water, but not water the way you’d pour it from a tap. This water is adherent to biological matter. It has charge. The proteins and cells in your blood also have charge. These charges interact, attract, repel. The interactions are integral to the function of circulation.
Now consider the red blood cells themselves. They carry hemoglobin. Hemoglobin carries oxygen. This much you know. But here’s what most people don’t know: hemoglobin is built around a structure called a porphyrin - a complex cyclic organic compound whose primary function is to absorb light energy and make it available to the body. Each porphyrin is a fiber-optic node doped by iron.
Let that sink in.

These are same class of molecule that give plants the ability to perform photosynthesis (using Magnesium instead of Iron) is sitting at the core of every red blood cell in your body.
The heme in your red blood cells (heme B) is not dramatically different from chlorophyll. Plants absorb sunlight to make food. Your mitochondria run an electron transport chain that is also heme-dependent.
What this means, practically, is that the vast majority of your blood - between the structured water and the hemoglobin - is a medium that harnesses, stores, and transmits light and electrons. Oxygen is the terminal electron acceptor of the electron transport chain. Its job is to create an outlet for the electron flow that produces ATP (energy).
The whole path looks like this:
Food provides electrons.
Light excites the electrons.
Oxygen closes the circuit and draws electron flow.
When you understand blood this way, you begin to appreciate why sources of natural light (i.e. near-infrared) have such a profound effect on circulation. This is not alternative medicine. This is biophysics.
Think of it this way.
The lungs are a portal system where your blood exchanges gas.
The liver is a portal system where your blood exchanges nutrients and clears waste.
The skin is a portal system too. It exchanges light of all sorts of wavelengths.
Sun, air, water. When you understand the skin this way, spending time outdoors stops being a lifestyle preference and starts being a physiological requirement.
Part III: How Blood Actually Flows
The heart does not pump blood the way you imagine a hydraulic pump.
Since William Harvey described the circulatory system in the 16th century we have held a model of the heart as a four-chambered organ that passively fills with blood and forcefully contracts to push it out. This is the model taught in every medical school on earth.
Dr. Francisco Torrent-Guasp changed that picture.
Paco, as he was known, demonstrated through meticulous anatomical dissection that the heart is not four discrete chambers acting in concert. It is one long muscle twisted upon itself like a rope. This muscle undergoes something more akin to peristalsis than pumping. The same coordinated muscular wave that moves food through your intestine moves blood through your heart.
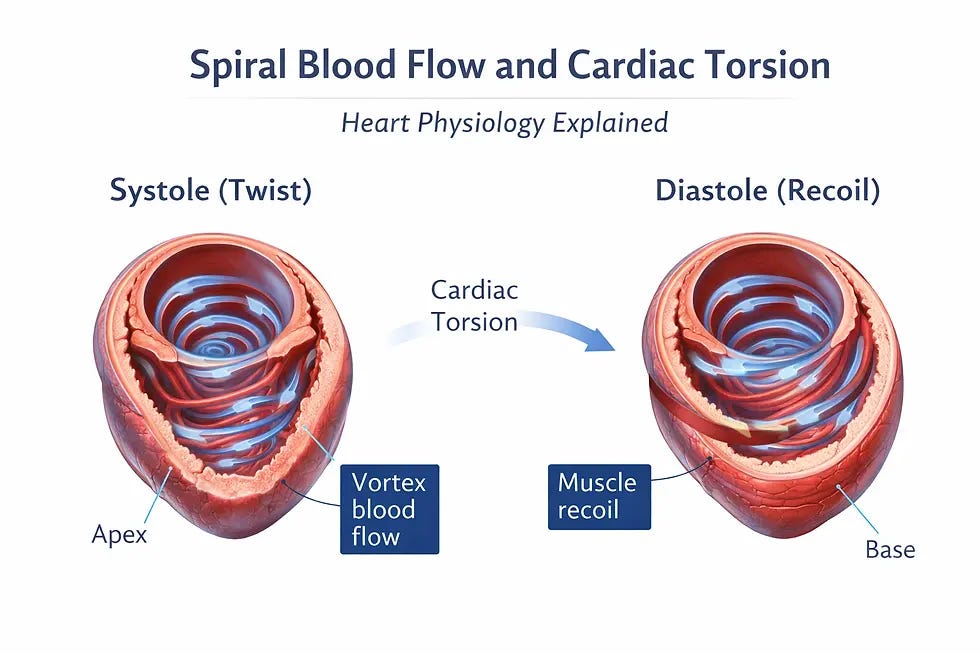
As blood moves inward, the apex contracts and ejects blood through the aorta while simultaneously drawing the basal loop back…creating a sucking force. Galen observed this and described the heart as “robbing the vena cava by violence of considerable quantity of blood” at each diastole.
It does this by creating a vortex: a tapering cone of rotating fluid that gives the blood forward momentum before the final contraction ever happens.
Gerald Pollack’s laboratory has been studying what happens to blood flow when you remove the heart from the equation entirely. In experiments using chick embryo models, blood continued to flow for hours after the embryo had been euthanized. Not from residual pressure. Not from vascular contractions.
What Pollack’s group has shown is that the inner lining of blood vessels creates what they call an exclusion zone: a structured layer of water, negatively charged. Red blood cells are also negatively charged. Like charges repel. This electrostatic interaction between the negatively charged RBCs and the negatively charged exclusion zone creates motion.
Pollack et al also observed that infrared light broadens this charged water boundary, amplifying the effect. The blood moved with more vigor in the dead animal after application of infrared light.

The blood moves, in part, because of light.
One final point on flow which connects directly to blood pressure.
Our circulation is a parallel circuit. Blood flows from the aorta into parallel pathways - arteries branching into arterioles branching into capillaries - each supplying different organs, muscles, and tissues. In a parallel circuit, the total resistance across the system depends on the resistance of each individual branch.
What happens when a branch is no longer used?
An organ that is chronically underused, or chronically diseased, reduces its blood supply. The vessels feeding that organ shrink, stiffen, or disappear. The branch closes.
KEY: in a parallel circuit, removing a branch increases total resistance.
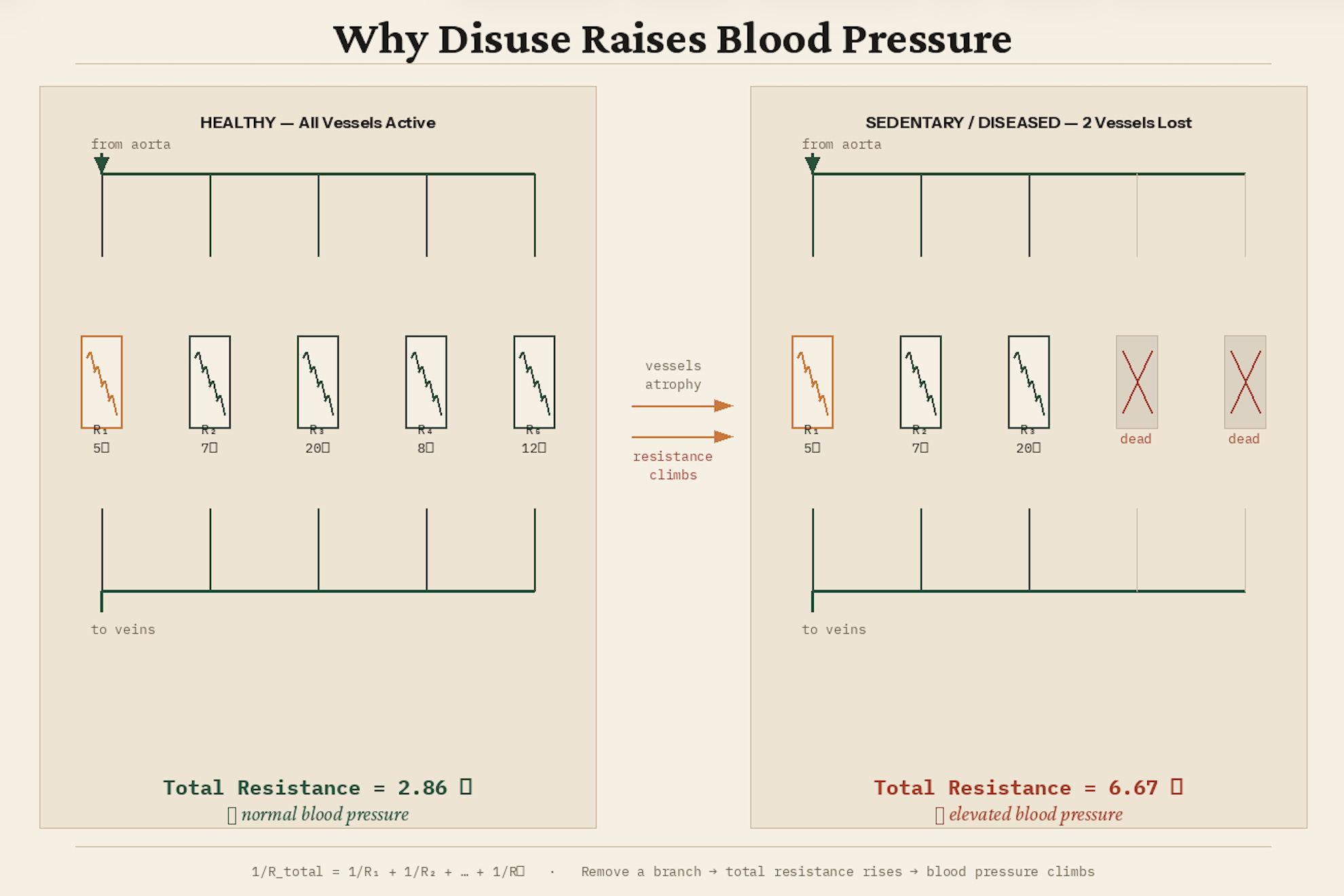
Higher resistance requires a higher pressure to maintain the same blood flow across the circuit.
This is why chronic sedentary behavior creates the conditions for elevated blood pressure over time.
More importantly, study after study (discussed below) demonstrates that being active results in better outcomes than blood pressure medications, irrespective of whether or not blood pressure is in a “normal” range.
Part III: The Diagnosis Dilemma
Now that you understand what blood is and how it flows, I want to turn to the way we diagnose and treat high blood pressure. Because this is where I think modern medicine fails people most.
Let’s start with the number.
When I began my medical education, systolic blood pressure between 130–139 was considered pre-hypertensive. A warning, not a diagnosis. By the time I finished training, those same numbers were Stage 1 Hypertension. A formal clinical entity. A justification for prescriptions.
The threshold did not move because the biology changed. It moved because guidelines changed. And guideline committees have a complicated relationship with the industries that benefit from lower diagnostic thresholds. This is a well-known phenomenon.

The United States currently uses hypertension thresholds that are meaningfully stricter than the European guidelines and the International Society of Hypertension. The same number, in the same person, results in a different approach depending on your zip code.
Now let’s talk about what we’re actually measuring.
When you get your blood pressure taken, the cuff goes on your arm - usually over the brachial artery. This is done because the brachial artery is the closest accessible vessel to the aorta. The assumption is that brachial pressure reflects central aortic pressure.
It doesn’t. Not reliably.
The brachial artery frequently overestimates central systolic pressure. In young adults (men > women) this discrepancy is widest.

Which means a young, otherwise healthy person can walk into a clinic, have a blood pressure of 135/82 measured in their arm, be diagnosed with Stage 1 Hypertension. Crucially, their central aortic pressure may be completely normal.
This matters for millions of people being placed on medications they may not need.
And about those medications.
Two large studies are worth your attention here. The first, by Brown and colleagues in 2013, tracked over 10,000 people across groups divided by activity level:
medicated and controlled (blood pressure),
medicated and uncontrolled,
unmedicated and uncontrolled, and
normotensive
Activity was, by a wide margin, the most powerful determinant of mortality. Being active with uncontrolled hypertension produced better outcomes than being treated, controlled, and inactive. The gap between active and inactive groups dwarfed the gap between medicated and unmedicated groups at nearly every point on the curves.
One of the more disturbing findings in this study is that the worst outcomes were in people who were not active, had uncontrolled blood pressure, and were on medication.
A 2022 JAMA publication extended this picture. The investigators looked at all-cause mortality, cardiovascular mortality, and cancer mortality across different combinations of lifestyle score and medication use. Their finding: at equivalent lifestyle scores, those not taking medication tended to achieve better risk reduction than those who were. And every additional increment of lifestyle improvement produced greater benefit in the unmedicated group.
Suppression of the signal (elevated blood pressure), without any meaningful improvement in the conditions which give rise to the elevated blood pressure…has consequences.
I am not telling you to stop taking your medications. I am saying that individual circumstances are infinitely variable.
You do not *have* hypertension.
Your blood pressure is elevated.
Those are not the same thing. The question is: why.
If you’ve followed the logic this far, you already know that lowering a number isn’t the same as treating a person. What follows is how I actually think about this and what I did when it mattered most.
If you want to tag along the journey or support this work, consider these options:
Monthly Member:
Complete essay archive access
Early podcast episode releases
Discount on future services
Founding Member (Limited spots):
Monthly +
Higher discount on future services
Join LIVE podcast recordings and ask questions
Receive guest list in advance and send questions to be asked
Part IV: The Case Study
I bring up this case again because it’s the perfect illustration of how the individual determines the path to resolving dysregulation.
So, let me tell you who my mother is before I tell you what her blood pressure was.
She is a Type A personality. A workaholic, in the truest sense - someone who works because she cannot stop. She is the kind of person who gives to everyone around her and treats her own needs as an afterthought, if she treats them at all. She runs on coffee and urgency. She doesn’t hydrate well. She doesn’t rest well. She has spent decades pouring herself out for other people and has never quite learned how to receive the same care she gives so freely. She’s getting better at that though.
If you were to ask the right questions:
who is she, and
why would her body manifest elevated blood pressure?
…the answer would be obvious before you ever took her blood pressure. Of course her pressure is elevated. Look at who she is.
