

the problem we didn't know to look for when we gave all newborns Vitamin K injections.
I have a theory, and we SHOULD NOT inject every newborn for vitamin K.

Whenever a baby is born in a hospital in North America, within 6 hours they are given a vitamin K injection. This is to prevent Vitamin K Deficiency Bleeding.
Remember the choice of words used to describe this phenomenon.
We give vitamin K not because we are concerned about any little bleeding that can happen in a newborn. We are worried about the type of bleeding that can end the life of a baby or leave them severely disabled.
In up to 60% of cases, this is related to a brain bleed.
Before we get into the framework used to describe this problem, as well as the real benefit of this intervention…let’s give the devil its due.
This is one of the longest articles I’ve written, so an overview:
The data in favor of vitamin K injection
What the stats hide
The population of newborns that benefit from vitamin K
What the above means for the true value of vitamin K injections
Why are babies born with low vitamin K?
My Hypothesis
what can happen if we “correct” low vitamin K
The data supporting the hypothesis
Those last 2 points are important, because as far as I can tell…there is no published literature making this hypothesis, and linking the hypothesis to vitamin K and the observed trends in childhood disease.
Which makes this article completely novel, and invites (even requires) immediate feedback to improve the hypothesis.
We begin with the strongest possible argument in favor of giving every newborn a vitamin K injection at birth. We’re going to present the numbers as favorably as the evidence allows. We’re going to assume the best-case scenario. And we’re going to be honest about what those numbers actually mean.
The Numbers Supporting Vitamin K Injections
First, a description of Vitamin K deficiency bleeding (VKDB) straight from the CDC.
Vitamin K is a substance that our body needs to form clots and to stop bleeding. We get vitamin K from the food we eat. Some vitamin K is also made by the good bacteria that live in our intestines. Babies are born with very small amounts of vitamin K stored in their bodies, which can lead to serious bleeding problems if not supplemented.
VKDB occurs when babies cannot stop bleeding because their blood does not have enough vitamin K to form a clot.
If you read that last sentence again, you will notice that VKDB is a disease in which something doesn’t stop. That is, when bleeding doesn’t stop.
Unlike the name suggests, it’s not a form of bleeding…it’s just bleeding in the setting of low vitamin K.
Simply: if bleeding doesn’t stop and you have low vitamin K = VKDB.
Even more circularly, VKDB is the condition vitamin K prophylaxis is designed to prevent. It has three forms: early (within 24 hours), classical (days 2–7), and late (weeks 2–12). The severe form we are worried about is late VKDB, which presents as intracranial hemorrhage in 30–60% of cases.
In high-income countries, among infants who receive no vitamin K prophylaxis, the rate of late VKDB is approximately 8.8 per 100,000 births. This is the median figure from a systematic review; the upper bound of the interquartile range reaches 17.8 per 100,000.
A single intramuscular injection of vitamin K at birth reduces this rate to less than 0.2 per 100,000. The relative risk reduction is approximately 98%.
The relative risk of developing late VKDB without prophylaxis is 81 times higher than with it.
These are the numbers you will find in every public health document, every AAP guideline, every CDC fact sheet. They are accurate. They are also, in isolation, profoundly misleading.
What the Relative Risk Conceals
When a relative risk of 81 appears in a policy document, it implies a large and urgent effect. It does not tell you how large the baseline risk is.
The absolute risk reduction from vitamin K prophylaxis in a healthy, term infant born in a high-income country is approximately 8.6 cases of late VKDB per 100,000 births. (8.8 - 0.2 = 8.6 per 100,000)
Not all of those cases result in death or permanent disability. Intracranial hemorrhage occurs in approximately 50% of late VKDB cases. Of those, in high-income settings with immediate NICU access, approximately 20–25% die and approximately 50–70% of survivors sustain permanent neurological injury. When you account for these figures, it’s less than 8.6 per 100K.
Optimistic scenario: number of newborns needed to inject (NNT) to prevent one death or case of permanent disability is between 27,000 and 33,000.
To prevent one catastrophic outcome, you must inject approximately 30,000 babies.
Using the upper bound of the risk estimate — 17.8 per 100,000 instead of 8.8 — the NNT improves to roughly 15,000 to 18,000.
Let’s grant this more favorable figure for the remainder of the argument.
This is not a criticism of vitamin K prophylaxis per se. An NNT of 15,000–33,000 can be entirely justified for a cheap, safe intervention with no downside.
But the question I pose, is whether the cost of mass-injection is zero…
The Population This NNT Applies To
Before examining the other side of the ledger, we need to be precise about which infants the best-case scenario actually describes.
The figure of 8.8–17.8 late VKDB cases per 100,000 in high-income countries without prophylaxis is a population-level estimate. It includes every birth in those surveillance populations — medicated and unmedicated, instrumental and spontaneous, induced and physiological. It is not the rate in the lowest-risk population. It is the average.
The lowest-risk infant for VKDB looks something like this:
Term gestation. Premature birth increases hemorrhagic risk substantially.
Healthy mother, no medications. Maternal anticoagulants, anticonvulsants, and antibiotics all increase neonatal VKDB risk.
Spontaneous, unmedicated vaginal delivery. Instrumental delivery and induced labor create specific risk factors for hemorrhage.
Exclusive breastfeeding from a nutritionally replete mother. Formula-fed infants receive supplemental vitamin K in formula and have substantially lower late VKDB rates.
No underlying liver disorder. A Dutch nationwide study found that the majority of late VKDB cases in their well-nourished population occurred in infants with underlying bile-static liver disease. Not in healthy infants.
Strip out the iatrogenic (caused by healthcare) and pathological risk factors, and the residual VKDB rate in a genuinely healthy term infant born via unmedicated natural delivery to a nutritionally strong mother approaches the lower end of the risk estimate. Maybe even less.
The Hospital Birth Environment as a VKDB Risk Factor
Here is what is almost never acknowledged in discussions of vitamin K prophylaxis: the modern hospital birth environment is itself a source of bleeding risk that does not exist under natural birth conditions.
The NNT figures cited above are derived from populations born in an unfamiliar and often times harmful environment. Just ask any doctor that works in a hospital: is a hospital a benign environment for a patient?
You cannot apply the same risk factors to natural births without accounting for the risks the hospital introduces:
Artificial, short range, constant light exposure. Vitamin K is degraded by ultraviolet and blue-spectrum light. Hospital lighting, particularly in NICUs and delivery rooms, delivers continuous artificial light exposure to a neonate whose plasma vitamin K levels are already low. The photo-degradation of vitamin K under clinical lighting conditions is documented in pharmacy literature. This is why vitamin K solutions are stored in amber vials. The effect of continuous blue-light exposure on an already low neonatal vitamin K reserve is not zero.
Cold environment and thermoregulatory stress. Hospital delivery rooms are maintained at temperatures comfortable for staff, not for newborns transitioning from 37°C intrauterine environment. Cold stress activates the sympathetic nervous system, increases catecholamine release, and alters peripheral vascular tone and coagulation dynamics in the neonate. Natural births in warm environments do not impose this stress.
Lithotomy position during delivery. The dorsal lithotomy position (on your lower back, legs elevated) is bio-mechanically awful for the delivering mother and infant. It prolongs labor, increases risk of tearing, and alters the pressure dynamics of delivery in ways that increase mechanical stress on the fetal head. Head trauma during delivery is a direct risk factor for intracranial hemorrhage.
Synthetic oxytocin (Pitocin) induction and augmentation. Synthetic oxytocin produces uterine contractions that differ from normal contractions: longer, more frequent, and lack the natural relaxation phase that allows fetal recovery of cerebral perfusion between contractions. The synthetic hyper-stimulation increases risk of unnatural cranial stress during delivery. Both hypoxia and cranial compression are independent risk factors for neonatal intracranial hemorrhage.
Instrumental delivery: forceps and vacuum extraction. Forceps and vacuum extraction apply direct mechanical force to the fetal skull. Both instruments are associated with increased rates of cephalohematoma, subgaleal hemorrhage, and intracranial hemorrhage independent of vitamin K status. It may not be as commonly used today as it was in the past, but that suggests that these older practices caused inflation of newborn hemorrhage rates, altering the apparent efficacy of vitamin K administration.
Maternal nutritional depletion. Extended hospital admissions, fasting policies during labor, and the absence of nutritional support during prolonged periods of induced labor leave mothers depleted of multiple micronutrients including vitamin K at the time of delivery and in the early postpartum period. Breast milk vitamin K content, already low, is further reduced by maternal depletion. This is not a feature of a well-nourished mother delivering spontaneously at term.
What This Means for the NNT
The honest interpretation of the available data is this:
The NNT of 15,000–33,000 to prevent one death or permanent disability from VKDB describes a mixed population that includes infants exposed to the iatrogenic (healthcare-caused) risk factors above. Many of the VKDB cases captured in surveillance data occurred in infants exposed to one or more of these iatrogenic or environmental risk factors.
In a term infant born via natural spontaneous vaginal delivery to a nutritionally replete mother, in a warm environment, without synthetic oxytocin, without instrumental delivery, the baseline late VKDB rate is almost certainly lower than the population-level figure. The NNT (number needed to treat) in this population is probably way higher than 33,000.
We do not have the data to calculate the precise figure, because no surveillance study has been performed with these factors considered.
This is not an argument that vitamin K prophylaxis should be withheld from all infant. It is an argument that the risk it addresses is not uniform across the population, that the NNT in the lowest-risk population is unknown and likely way higher than cited figures. A policy of universal prophylaxis is treating a problem that modern obstetric practice substantially creates…without examining whether the treatment introduces problems of its own.
That examination is what the rest of this article is about.
Is there a downside to vitamin K injection?
With an NNT that high, the downside does not have to be huge to warrant deeper consideration.
So…what is the downside?
I think we missed something.
Why are Babies Born with Low Vitamin K?
Doctors have assumed for decades that this is a mistake of nature, a design flaw that needs to be fixed with an injection. This paper argues the opposite: nature made this choice on purpose. Nature intended that a newborn’s blood stays thin during the first hours and days of life because the baby’s body is doing something extraordinary: opening new and developing existing networks of blood vessels that have never had blood flowing through them before. Or had very little blood flow through them in the past.
If the blood clots too easily during this process, it could damage the very organs that are trying to develop with the vascular bed. When we give every baby a vitamin K shot, we may be interfering with a protective system that nature designed. And the evidence suggests we’ve been unknowingly paying a price for it.
Newborn babies are born with almost no vitamin K. This happens three separate ways:
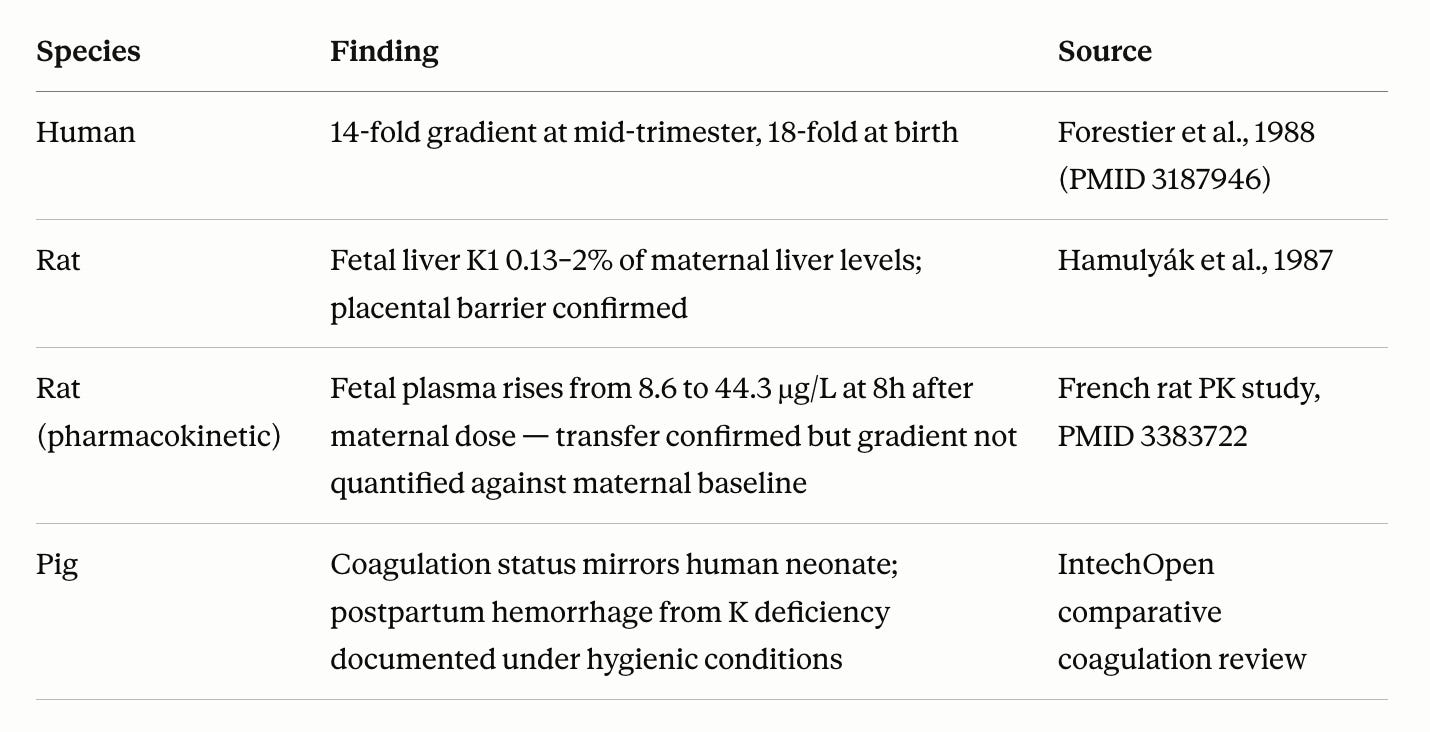
Vitamin K does not cross the placenta in any significant quantity.
Breast milk barely contains it. A breastfeeding mother can take vitamin K supplements every day and it still barely appears in her milk.
Newborn guts can’t make it. Adults make some of their vitamin K through bacteria in their intestines. Newborn intestines don’t have this bacteria.
Three completely separate systems all pointing in the same direction: keep vitamin K away from the newborn.
Doctors look at this situation and say:
“This is a deficiency. The baby is vulnerable to bleeding. We need to fix it.”
But here’s a different question: Why? Why is it low?
If one biological process leads to low vitamin K, you might call it an accident. If two systems did it, you’d start wondering.
But, when three independent systems all converge on the same outcome, the probability that it’s an accident becomes very low.
And, as far as we know from the veterinary literature, it is not uncommon among mammals with a placenta:
So what would be the reason?
THE BIRTH EVENT
Think about what happens the moment a baby is born.

For nine months, the baby’s lungs were filled with amniotic fluid. Not air. The placenta was doing the breathing. Less than 10% of the heart’s output went to the lungs. In adults its 100% except for the blood that goes into the coronary arteries.

At the first breath:
The lungs expand for the first time
Blood rushes into the lung circulation: the full output of the heart.
The liver, which had been getting blood from the placenta through a shortcut, now has to process all the blood through tiny internal channels for the first time.
Shunts that bypassed organs in the fetus begin to close.
This is the most extreme cardiovascular event in human life, compressed into seconds, minutes, hours, days.
The Problem: Opening Up Empty Pipes
When blood first rushes into a system of vessels that has never had flow before, there’s a problem:
Slow-moving, low resistance blood flow tends to clot.
This is a direct consequence of Virchow’s Triad, named after a 19th-century German doctor who figured out the three things that cause blood clots:
Blood moving too slowly (or not at all)
Damage to the vessel wall
Blood that clots too easily (e.g. too many clotting factors)
The new blood vessels being recruited in a newborn’s lungs, liver, and brain satisfy at least the first condition automatically: there’s a window of time before normal flow is established where the blood is sluggish. And in these same vessels, the walls haven’t yet been trained to resist clotting (more on that below).
If the blood clots too easily during this recruitment window, the developing vessels get blocked. Not catastrophically, this is a developing organ. It mostly disrupts/changes the architecture. But it can have effects in severe cases. As we will discuss below.
Blood Vessel Walls Need to Learn to Resist Clotting
Here’s something remarkable about blood vessel linings: they only become anti-clotting once blood is flowing through them.
The inner lining of blood vessels (endothelium) responds to the physical force of blood flowing past it. When blood flows steadily, the vessel wall releases signals that actively prevent clotting.
But that’s after laminar (not turbulent) blood flow has been established.
So in the critical window when new vessels are opening up and trying to recruit flow, the walls of those vessels are pro-clotting until they learn otherwise.
The only systemic protection available during this window is: blood that doesn’t clot easily.
Which is exactly what low vitamin K provides.
THE THREE PLACES THIS MATTERS MOST
1. The Lungs
The lungs don’t finish developing at birth. The tiny air sacs (alveoli) and their surrounding blood vessels continue forming in the first weeks and months of life. Specialized cells in the lung’s capillary network are actively dividing and building new exchange surfaces after birth.
If tiny clots form in the capillaries being recruited into this new architecture, the alveoli don’t get the blood supply they need to develop properly. The result: simplified lung structure, reduced gas exchange capacity, structural vulnerability.
This is essentially what bronchopulmonary dysplasia (BPD) looks like.
")
Look at what BPD manifests as. The sac are malformed, and dysplastic. To me, these lungs look like they may be quite reactive to irritants or toxins.
These hypersensitive lungs can manifest as something like asthma.
2. The Liver
Before birth, the liver had a shortcut: blood from the placenta could bypass most of the liver’s internal filtering system through a vessel called the ductus venosus. At birth, this shortcut closes. All the blood that enters the liver must now flow through a vast network of tiny channels for the first time.
These sinusoidal channels are still developing their final structure when birth occurs. Subtle thrombosis here during first recruitment could disrupt architecture in ways that manifest years later as metabolic dysfunction, elevated liver enzymes, or portal hypertension.
3. The Brain. Yes.
The area around the brain’s ventricles (periventricular region) is fed by tiny end-arteries with no backup blood supply. This region is actively being built when a baby is born, populated by the cells that will eventually form the brain’s white matter: the information highway. Defects here lead to slowing in information transfer, at the very least.
This network is part of a matrix (germinal matrix) that are the most fragile cells in the developing brain. They are exquisitely sensitive to being cut off from blood supply, even briefly.
If the periventricular capillaries experience even minor disruption (clots) during development, these precursor cells die or fail to mature. The result: white matter never gets properly developed. Brain circuits don’t connect properly. This is called periventricular leukomalacia.

This is the architecture and imaging finding associated with cerebral palsy, and increasingly, autism.
Evidence 1: The Lung Numbers
Doctors have been giving vitamin K to all newborns since 1961 in the United States. Adoption was gradual, reaching near-universal coverage by the late 1960s to early 1970s.
The first generation of fully prophylaxed babies started generating neonatal and childhood outcomes data in the 1970s and 1980s.
What happened to bronchopulmonary dysplasia rates in that exact period? They tripled. From 10.6% to 32.9% of very low birth weight babies over a single decade. With the same diagnostic criteria. With known risk factors analyzed and ruled out as explanations.
Nobody has adequately explained this.
Evidence 2: The Same Pattern in Brain
Cerebral palsy rates rose from 1.68 per 1,000 babies in 1964–1968 to 2.45 per 1,000 in 1989–1993. This rise was documented not just in premature babies, but also in full-term babies. That’s the important part.
Full-term babies have no prematurity to blame.
Nine separate international registries all showed the same trend: rising cerebral palsy through the 1970s and 1980s.
Evidence 3: The Smoking Gun
Here’s the most striking finding.
Brain bleeds in premature babies has dropped from 50% of very premature infants in the 1970s to 15–25% today. Vitamin K prophylaxis is partly credited for this. Less bleeding. Good.
But here’s the problem: neurodevelopmental outcomes didn’t improve in proportion. The babies stopped bleeding, but the brain damage didn’t stop.
The type of damage changed.
Instead of obvious hemorrhage, there is an increasing trend of white matter lesions likely due to non-bleeding, ischemia/clot related damage that’s harder to see on traditional scans and that directly causes myelination failure and connectivity deficits.
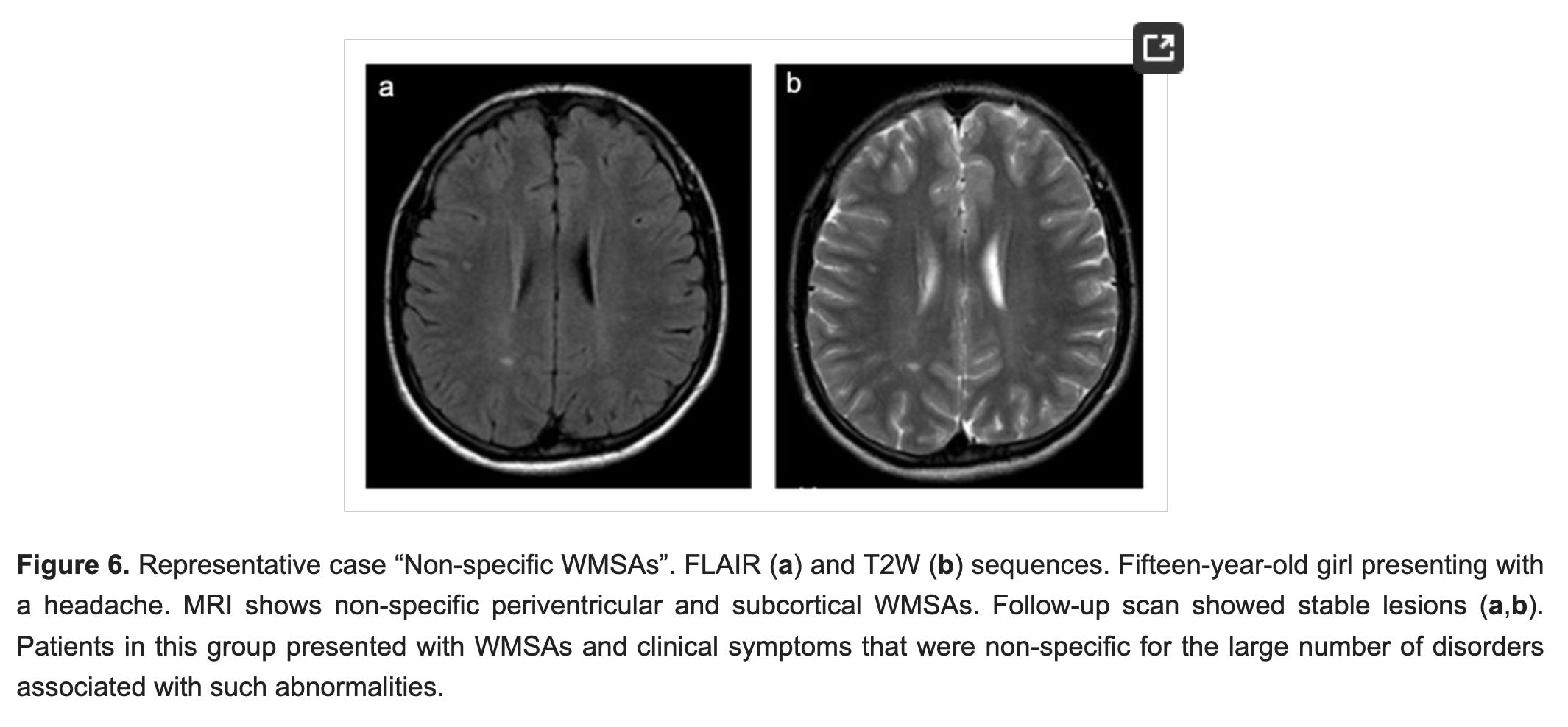
Less hemorrhagic damage. More thrombotic damage. Still brain damage.
This is exactly what we’d predict would happen if you suppress the thin-blood phenotype (by normalizing vitamin K), without addressing the underlying vulnerability of newly recruited blood vessel networks.
Evidence 4: The Autism Connection
Children with autism spectrum disorder consistently show abnormalities in the white matter of the periventricular region, precisely the area most vulnerable to the mechanism described above. Studies using advanced MRI have found:
Elevated periventricular white matter injury markers in ASD vs. typically developing children
The amount of white matter injury correlates with the severity of ASD symptoms (specifically repetitive behaviors)
White matter abnormalities detectable in ASD children as young as six months old — meaning they were present at or near birth
Diffuse white matter injury is now recognized in the scientific literature as a risk factor for autism, ADHD, cerebral palsy, and learning disabilities. What nobody has proposed is what causes the white matter injury in the first place in babies who weren’t premature.

This hypothesis proposes a new answer: normalized coagulation during the blood vessel recruitment window.
To summarize: to prevent 1 catastrophic bleed after treating at least 20,000 infants…we are risking increasing rates of cerebral palsy (severe disability) and a spectrum of autistic disorders…at the very least.
There are probably other connections I haven’t yet looked for because this theory has only just been developed.
The Evidence Was Never Collected
Once vitamin K became universal in 1961, the comparison group was gone. You can’t study what doesn’t happen in a population where everyone gets the intervention.
The harms being proposed here are:
Delayed: injury at birth; consequences appear over years
Invisible at the time: you can’t see a tiny clot in a periventricular capillary in a newborn in 1965 (hard to see even today).
Diffuse: not one dramatic event, but architectural disruption across millions of tiny vessels.
Attributed elsewhere: the child with cerebral palsy or autism gets their diagnosis years later, with no connection drawn back to what happened in their first hours of life
In 60+ years of vitamin K literature, I don’t think anyone has proposed that neonatal vitamin K deficiency might protect newly developing blood vessels. The literature only describes the deficiency, characterizes it as a problem, and studies how to correct it.
THE BOTTOM LINE
Nature arranged for every newborn to have low vitamin K. Three separate biological systems cooperate to ensure this. The most extreme cardiovascular event in human life (when the lungs, liver, and brain all open their blood vessels for the first time) happens in this low-vitamin-K window.
We have overridden this arrangement for 60 years, universally, for every baby born in the developed world.
The epidemiological record (rising rates of lung disease, brain injury, and neuro-developmental disorders in the first generation of universally prophylaxed babies) is consistent with the possibility that vitamin K is low for a reason.
Not deficient.
References
Sankar MJ, Chandrasekaran A, Kumar P, Thukral A, Agarwal R, Paul VK. “Vitamin K prophylaxis for prevention of vitamin K deficiency bleeding: a systematic review.” Journal of Perinatology. 2016.
Sinkin RA, Cox C, Phelps DL. "Predicting risk for bronchopulmonary dysplasia: selection criteria for clinical trials." Pediatrics. 1990.
Jobe AH, Bancalari E. "Bronchopulmonary dysplasia." Am J Respir Crit Care Med. 2001.
Colver AF, Gibson M, Hey EN, Jarvis SN, Mackie PC, Richmond S; North of England Collaborative Cerebral Palsy Survey. "Increasing rates of cerebral palsy across the severity spectrum in north-east England 1964–1993." Archives of Disease in Childhood — Fetal and Neonatal Edition. 2000.
Scheller JM, Nelson KB. "Timed relation of a single seizure to perinatal factors in neonates." American Journal of Obstetrics and Gynecology. 2003.
Georgiadis P, et al. "White matter injury in infants with intraventricular haemorrhage: mechanisms and therapies." Nature Reviews Neurology. 2022.
Blackmon K, Ben-Avi E, Wang X, Pardoe HR, Di Martino A, Halgren E, Devinsky O, Thesen T, Kuzniecky R. "Periventricular white matter abnormalities and restricted repetitive behavior in autism spectrum disorder." NeuroImage: Clinical. 2015.
Bronchopulmonary dysplasia as a risk factor for asthma in school children and adolescents: A systematic review." Allergologia et Immunopathologia. 2017
💯👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏👏🎩
Wow, excellent research! If only I could go back. My older son has asthma and adhd. No idea if it was due to the K shot or the vaccines or both, but I’d undo every last unnecessary medical intervention if I could do it over. I have learned so much since my kids were born (early nineties) It was all risk and no reward 😢