

INSIGHTS | 20. The Link Between Autism & Inflammation
Neuroimaging allows us to look inside that infinitely complex structure we call the brain. Unfortunately, this isn't routinely done for those with Autism.
Article: Normal Rates of Neuroradiological Findings in Children with High Functioning Autism

Background
In recent years, people have become justifiably skeptical about Big Pharma and vaccines. With recent covid policies, the definition of “anti-vaxxer” has expanded as well.
When I was in school, an anti-vaxxer was characterized as someone who thought the MMR vaccine caused autism. But recently, our regulators have expanded this definition to include anyone opposed to vaccine mandates.
Quite the range of beliefs for one derogatory term.
But, this article is not about vaccines.
This piece is about the role of inflammation in neurological disease, with attention on autism.
What is Autism?
The definition and diagnostic criteria for autism should help illustrate how incomplete and uncertain a condition it really is. Initially, people would refer to those with difficulties in language & social interaction as autistic.
Now, we refer to it as autism spectrum disorder (ASD) because, over time we learned that it wasn’t as simple as we thought.
The most recent Diagnostic and Statistical Manual of Mental Disorders (DSM-5) has very elaborate diagnostic criteria:
Persistent deficits in social communication and interaction
Restricted or repetitive patterns of behavior, interest or activities
Symptoms must be present in early developmental period
Symptoms cause impairment in social, occupational, and life settings
Not better explained by intellectual disability or global developmental delay…
But, intellectual disability frequently co-occurs with ASD (go figure)
The DSM goes on to state that the doctor must specify if there is:
Intellectual impairment
Language impairment
Developmental, mental, or behavioral disorders
Catatonia - abnormal muscle tone
Associated with medical or environmental factors
It’s all a bit complicated.
What is Autism, really?
One of the best descriptions I have come across was from Karl Deisseroth, who was a guest on the Lex Fridman podcast. Karl is best known for his pioneering work on optogenetics, but is also a psychiatrist.
In Karl’s view, autism is an inability to appropriately process new information.
You may be wondering ‘what is the connection between social interactions and processing new information?’
As Karl points out, since autistic people have difficulty processing novel information, the domain within which that would manifest the greatest is social dynamics. There is nothing as unpredictable, chaotic and idiosyncratic as interactions with other humans.
Thus, it would make sense for the most apparent ‘deficiency’ within autism to be social interaction. A natural extension of this would be language fluency and intellectual disability.
What causes Autism?
You can find an extensive list of possible causes for Autism, but fundamentally we do not know. It is almost certain that if ASD represented a unique disease, it would have multiple causes.
If you think about the fundamental problem (as described by Deisseroth), slow processing of novel information, it isn’t difficult to imagine the possible causal or contributory factors.
For example: maternal nutritional status, pre-natal and perinatal factors, complications during birth, immunologic & inflammatory stress during infancy, exposure to toxins, lack of cognitive support & nourishment during early years, poor behavior modelling, and so on.
I believe there are two factors that are often ignored with autism:
Poor behavioral modeling, and its impact across generations - to be written about in a future article.
Overall inflammatory state and the impact this has on anatomy and physiology of the brain - the topic of this article.
The Normal Brain
An MRI is useful because it allows us to look at the brain with exceptional contrast resolution. The stronger the magnetic field, the higher the resolution - generally speaking.
Here we have a T2-weighted image of a normal brain:

Notice a couple of things:
Gray matter is gray (ribbon of cortex along the periphery)
White matter is really dark - especially near the top of the image (which corresponds to the frontal lobes)
Normal cerebrospinal fluid is bright white - in the sulci between the cortical gyri, and within the lateral ventricles at the center of the image.
The problem with a T2-weighted image is that all fluid will be bright, making it difficult to differentiate between normal fluid and pathological fluid.
This is what a FLAIR sequence is for. It suppresses normal fluid, so all that is left is pathologic fluid, if there is any.

Notice in the above normal FLAIR sequence:
Gray and white matter are whitish-gray and dark, respectively - like T2 image
This time, the normal CSF within the sulci and ventricles are suppressed - so they appear dark
The above images were most likely taken with a 1.5 Tesla strength magnet.
Bonus: Look what happens when we crank this up to 7 Tesla - beautiful isn’t it?

The Inflamed Brain
If you are looking for a pathologic lesion, you are most definitely getting a FLAIR sequence. A common location for chronic lesions is the white matter - the connective tracts of the brain.
Rarely is there a pathologic diagnosis of the brain which does not manifest with lesions in the white matter, which are visible on FLAIR.
But, what does it mean for there to be a white matter lesion?
They can result from several things:
Demyelination - like with multiple sclerosis
Gliosis - fancy word for scarring
Infarction - such as from strokes or bleeds
Disease of the veins which alters perfusion and drainage
Inflammation - systemic or focal
Infection
Tumor
As the brain experiences inflammation the person will manifest neurological symptoms. If it is acute and severe, the person may become comatose.
If the inflammation is low-grade and persists chronically, then corresponding regions of the brain will start to develop features like scarring, volume loss (prolonged ischemia), bleeding, demyelination, and swelling.
Exhibit A. FLAIR sequence of a person with multiple sclerosis - a demyelinating disorder:

Look at all those white blotches in locations including: surrounding the ventricles, in the deep white matter, and the subcortical (more specialized regions) white matter.
Imaging Autism
Since genes are a common way to look at illness, outdated perspectives on autism included assumptions about its genetic basis and heritability.
So, the early attempts at characterizing the imaging findings of ASD looked at major heritable anatomic differences. This early research was often done with computed tomography or low resolution MRIs - making finer anatomic differences difficult to distinguish, if not impossible.
Consequently, the American Academy of Neurology, the American Academy of Child and Adolescent Psychiatry, and the American Academy of Pediatrics have independently concluded that imaging is not indicated as part of the routine evaluation of children with autism.
More recent research, which has not made its way into diagnostic or management algorithms within fiat medicine, uses higher resolution imaging.
These studies reveal more interesting pictures.
For example, Boddaert et al look at MRI of 69 children with ASD and 77 normal. In ASD, distinct abnormalities were found including: 27.5% had white matter lesions and 29% subcortical lesions & infarcts within the temporal lobes.

Granted, not all studies show similar frequency of these lesions. The article linked at the top did not find a difference in kids with ASD. But, they also have differences in imaging technique and age-range, which may account for these observations.
Regardless, my assertion is not that these lesions explain all cases of ASD.
I argue that some of the symptoms may be explained by these lesions. They may even point to multiple contributing causes, which manifest in the global picture of ‘autism.’
Why White Matter Lesions?
The brain is a highly energy-intensive organ in a very confined space that happens to be on one polar end of your body - very far from the heart.

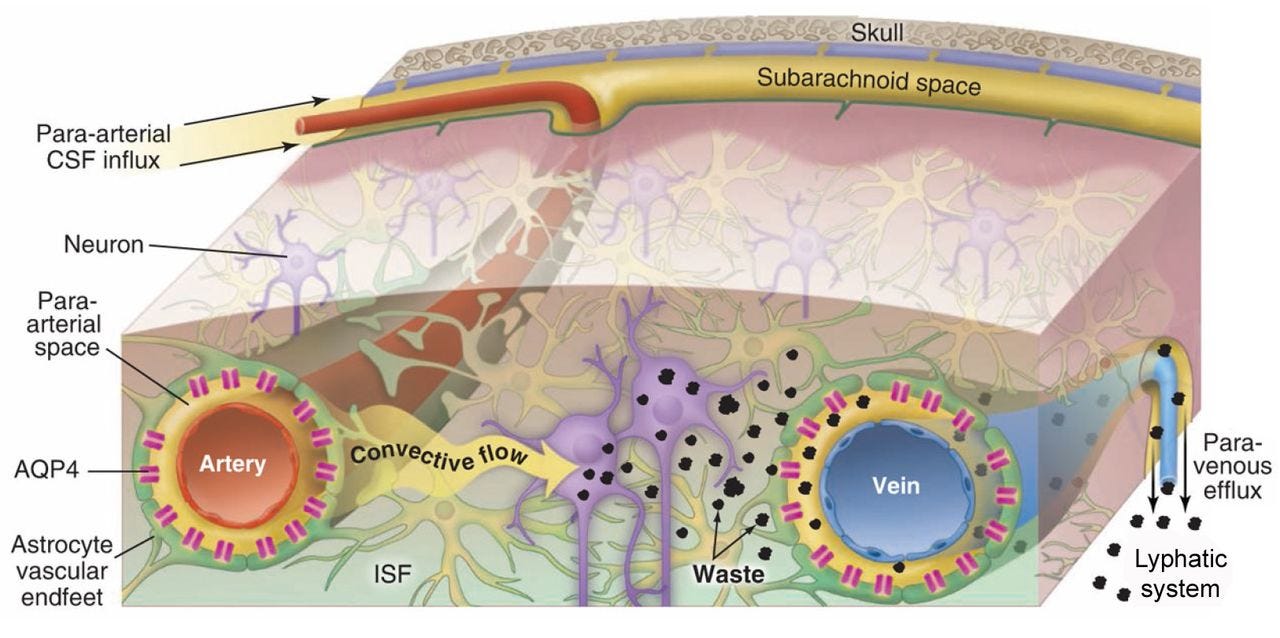
As you can imagine, it has a very finely balanced and regulated mechanism to maintain a robust supply of energy, metabolites, and oxygen to the brain. In addition, it also has a complex mechanism to clear waste from the brain.
We cannot have fluids & waste build up in such a confined space.
Consider how relatively simple the combustion engine in your car is compared to the brain. Now consider all the maintenance that needs to be done to make sure that the car is ‘firing on all cylinders.’ At minimum, you need to provide adequate fuel, have an efficient exhaust system, and make sure the engine lubricant is free of debris, waste, and degradation products.
In the brain, even chronic low-grade inflammation can impact the functioning of neurons as well as the integrity of the vasculature which nourishes and clears waste from the brain.
One of the factors which can have a significant impact on this, is diet.
However, anything that can impact the optimal functioning of the brain can:
Result in symptoms related to the region of the brain that is underperforming
If chronic, the pathology can result in chronic changes to brain structure
Implications
Practically, what does this mean?
For one thing, children are diagnosed with ASD very early in life. Timing matters. The sooner you intervene, the better.
The earlier the onset of symptoms or diagnosis, the more likely it is that a change in lifestyle may reduce symptoms and long-term consequences.
If we can pull a clot out of an artery fast enough, we can minimize the volume of infarcted brain in the event of a stroke. This is a very short time-horizon event.
Chronic low-grade inflamation provides a longer window of intervention.
So, the sooner you stop giving things to your children which can induce, prolong or worsen inflammation…the sooner you can stop progression and maybe recover some function.
But, what about vaccines?!
I am not here to argue about individual vaccines causing autism.
But, every vaccine depends on an immune response to work. They induce inflammation, both local & systemic, by necessity.
How many and how often do you need to vaccinate your child before the recurrent inflammatory cycles result in impact on the brain which may manifest with neurological symptoms?
How long until these structural changes become permanent?
At what age do you want to minimize this stress to optimize the uptake of social intelligence?
We haven’t even started talking about environmental toxins, diet, low activity, and social behavioral modelling.
These are the important questions.
Thank you for your support.
I think there are too many neurological diseases that have names that may be related with no physical evidence/cause. This is great for pharma not wanting to find causal effect since it would hurt their revenue stream. The Vaxxx schedule has become ridiculous as neurological issues increase. Dr Christopher Exley has found toxic aluminum in brain biopsies of autism and alzheimer patients. 42 out of 45 vaccines have aluminum adjuvants. Based on Dr Robert Vogel study May 2025 the average adult male consumes over 4lb of aluminum in food and drink annually. Call me crazy but this is more evidence than pharma will come up with. But I think you are correct there are many causal effects that are related to poorly undefined diagnoses. Dr Coimbra has had success battling autism with high dose D3 since it is required for the immune system and the brain and every other cell. DR Andreas Kalcker has had success reversing autism in one of his family members with chlorine dioxide. I was wondering if iodine deficiency would play a role since 80% of us are and iodine is required for every cell including the brain. Iodine is a defense but it is also required for cellular secretion. Since the brain replaces the cholesterol about every 10 months, having sufficient iodine and D3 for the brain may help.
Thanks for taking this on. My work is with nonspeakers, the bulk of whom are ASD individuals on the end of the spectrum with more/most significant disability. If the “spectrum” concept with ASD is even valid (I’m not sure it is), I know nothing about those on the more subtle end of the spectrum. I’m only speaking for the others….
I agree it’s important to recognize causality is likely complex and multifaceted.
I strongly disagree about your hypothesis regarding behavioral modeling. These disabilities are MUCH deeper and parenting styles are incredibly diverse. In fact, I think using a behavioral lense with ASD is inherently the wrong take.
The guys I work with have what people label as problematic “behaviors” but misunderstand these as purposeful. The guys I work with have a major sensory-motor difficulty. They can know what they want/mean to do with their bodies all day long and can’t make it happen without help. They have minds that are intact and bodies that have a “mind of their own.” The major feature of their disability is sensory/motor. (I know there are other global systemic issues like digestion and immune system issues associated with ASD but I’m talking about the “behavioral” aspects that are used to diagnose.)
The reason these things are known/understood to some degree is through acquired communication skills with letter boards. It is motor disability that makes communication initially out of reach and it is a painstaking process of myelinating ingrated skills of thinking and doing simultaneously that yield an ability for them to testify to what their disability on their level of experience. There is no deficit in language. Receptive language is completely intact. They understand everything people are saying with spoken words. Expressive language skills can always be expanded and grown through use for all of us (the more I try to use words to express myself the more skilled I get at that; this is true for everyone).
The behavioral framework is the wrong framework. One researcher who gets the importance of looking at the sensory/motor origin of how behaviors present us Liz Torres. (I forget what university she’s out of - pretty sure it’s in NJ but might be PA).