

Pharma's Alibi | The 15-Year S.M.O.N. Epidemic of Japan
An Epidemic swept through Japan from 1959 to 1973, but how come you have never heard of it? And what happened to the virus that caused it? This story is a reminder to keep our heads on straight.

In the Wake of Polio
In the 1950s, Japan was in the middle of a “war” on Polio. As such, there was a very active and well funded virological community - not unlike our own NIH.
In February 1962, Abraham Kaplan (Professor of Philosophy) gave a banquet speech at a conference of the American Educational Research Association held at UCLA. In June of the same year the Journal of Medical Education highlighted a comment by Kaplan on choice of research methodology. Referring to Kaplan’s Law of the Instrument:
Give a boy a hammer and everything he meets has to be pounded.
And so, this story begins.
The S.M.O.N. Epidemic
Reisaku Kono was studying poliovirus, which he had observed that in a few infected individuals would result in symptoms involving the central nervous system causing progressive paralysis and sometimes, death. In 1959, he observed the case of a middle-aged woman suffering from a mysterious illness that had paralyzed both of her legs. His suspicion was that this too may be the result of an as of yet unknown virus.
Hiroshi Takasaki, a professor of medicine at the university hospital caring for this woman, mentioned that he had recently observed a number of cases that were similar. In the previous year, professor Kenzo Kusui published a report of a similar case in central Japan. This patient had a combination of intestinal problems, bleeding, diarrhea, and nerve degeneration. This pattern was noticed in a few isolated cases in 1955. Kono now realized they were facing an outbreak of something new.
In the next five years, 7 major regional outbreaks of the new syndrome were observed. By 1964, 161 cases were identified. The observed growth had all the makings of an infectious outbreak.
Although the scientists who thought the disease might be related to an occupational hazard were dissuaded of the notion, some noticed important contradictions to the virus hypothesis.
the disease had a bias towards middle-aged women
less common in men
could hardly be found in children
Blood and bodily fluids showed no abnormalities
patients did not manifest systemic signs like fever, rash
To his credit, Kono noted “I was at that time engaged in poliovirus research, so I suspected such a virus to be the cause.”
However, with the 1964 Olympic Games approaching, the lack of isolated virus was little comfort to Japan. 96 new cases were diagnosed the previous year, and some people had new symptoms - like blindness.
That same year, during the 61st General Meeting of the Japanese Society of Internal Medicine this disease was given a formal name: Subacute Myelo-Optico-Neuropathy AKA SMON. The Japanese Ministry of Health and Welfare provided research grants, and launched a formal commission to investigate the epidemic, with Kono as one of several virologists named to the commission.
Virus Hunt begins
Shortly after, Masahisa Shingu announced his discovery of a virus in excretions of SMON patients - classified as an echovirus. Enteri Cytopathogenic Human Orphan Virus. Orphanbecause they had been discovered incidentally during polio research, but caused no disease. He speculated that like polio, this enteric virus could breakthrough into the nervous system. He published his finding in 1965.
After three years of research trying to confirm Shingu’s claims, Kono could only report to a SMON symposium that he could not isolate the virus from patients. Moreover, he could not even find indirect evidence that the patients had previously been infected.
During this period of investigation, the team made a rather surprising observation. About half of the patients with SMON has previously been prescribed a diarrhea medication called Entero-Vioform. Another half of the patients had received a drug named Emaform. Both drugs were prescribed for early symptoms of SMON - digestive problems. This was brushed aside, as two different drugs should not cause the same new disease - plus it was a virus anyway, for sure.
The commission dissolved in 1967, without an identified pathogen. Shortly after, two rural areas saw an outbreak in Okayama province. By 1971, almost 3 percent of the local population had developed it.
If at First you don’t succeed…
In 1969, the Japanese Ministry of Health and Welfare formed yet another investigative body. This time with more than 10x the funding of the original 1964 commission. SMON research became the largest Japanese research program ever devoted to a single disease. This time, Kono was named as Chairman.
Kono understood that he needed to pursue alternative hypotheses, so he divided the commission into four sections: epidemiology, virology, pathology, and neurology. In total, 40 of the nations top scientists participated in this commission.
Despite Kono’s efforts to pursue alternative causes, this did not stop the influence of outside research from English and American virologists. In the early 1960s, Carleton Gajdusek from the United States NIH reported finding evidence of the first “slow virus” - a disease produced long after the original infection, with a latency period.
Gajdusek believed that Kuru disease (affecting natives of New Guinea) was caused by a virus. Though his methods for ‘confirming’ a viral causes were questionable at best. He ground up the diseased brains of dead Kuru victims, and injected the mixture into the brains of living monkeys. When some of the monkeys developed the same symptoms, he published his findings in Nature. The problem is, Kuru is a prion disease - similar to Mad Cow. It is infectious yes, but not viral. It is transmitted by protein - proteins can be infectious.
The idea of infectious proteins was not known at the time, and so Kono could not ignore the assertion. Especially after it was published in the world’s oldest scientific journal- Nature. This plunged the SMON commission back down the “viral” rabbit-hole. Kono argued that if scientists could not entertain the idea of a non-classic virus, then “Dr. Gajdusek could not have etsablished a slow virus etiology for kuru.” In an attempt to imitate Gajdusek’s method, Kono tried the same with with fluids form SMON patients. He failed to reproduce symptoms. Then he sent samples to Gajdusek himself, who also failed. And so, Kono abandoned the search for a “slow virus.”
I want to take a moment in this story to praise Kono in his efforts. Despite the zeal with which he and his colleagues approached the virus hypothesis, when experimentation proved unsuccessful, he was completely willing to accept the results. This is not common in science or medicine. As it turns out, being a scientists is really hard, even for scientists.
A Non-infectious cause?
After 12 years of the virus hunt, research into the SMON epidemic yielded no identifiable cause. In 1969 the disease had claimed another 2,000 victims, the worst year yet. Thankfully, Kono had designed the commission with more than just virologists.
Dr. H. Beppu, a pharmacologist, visited Okayama in 1969 to investigate the outbreak and had made an eerily similar discovery. The SMON victims had taken certain drugs to treat diarrhea. Unlike the prior group, Beppu looked past the names Entero-Vioform and Emaform and discovered that these two were brand names for the exact same compound - Clioquinol. To test his hypothesis, he gave clioquinol to mice in hopes to recreate the nervous system damage in SMON. To his disappointment, the mice died.
In a rather comical exchange, his colleague Totsuka said “He later confessed to feeling stupid, because he gave up the experiment when the animals died,” adding “he wanted to prove a neurological disorder, but only proved the drug’s severe toxicity.” Clioquinol was used for intestinal parasites, like amoeba, because it was believed to remain in the intestines. The death of Beppu’s mice proved that the drug was absorbed by the body, and could kill.
Meanwhile, a nationwide survery of SMON cases were underway, and in the fall of 1969 the survey uncovered several patients with a strange green coating on their tongues - hitherto unnoticed by the literature. This was at first brushed aside as a Pseudomonas colonization, but quickly became prominent when in May of 1970, a group of doctors encountered two SMON patients with greenish urine. Shortly thereafter, chemical analysis of the urine revealed an altered form of clioquinol.
The Machine resists
You would think that this discovery would pave the way for a rethinking of the cause of SMON. From contagious to non-contagious. But you would be underestimating the degree to which humans influence science and medicine.
The idea that clioquinol was the guilty party was met with even stronger resistance, because it was the very drug that doctors had been using to treat SMON patients for years. Doctors were reluctant to believe that they were making the problem worse, and causing severe nervous system damage. Doctors ignorant of clioquinol’s side effects assumed the stomach pains resulted from the elusive primary sickness and kept increasing the dose in a vicious cycle.
The group knew they had to gather strong evidence before the virus hypothesis could be shot down. By july of 1970 their data analysis revealed:
96% of SMON victims had definitely taken clioquinol before the disease appeared
those with the most severe symptoms had takent he highest doses of clioquinol
Number of SMON cases throughout Japan had risen and fell with the sales of clioquinol
The clioquinol hypothesis explained far more than the elusive virus-hunt ever did:
Preference for striking middle-aged women
near absence in children (who would have recieved fewer and smaller doses)
tendency to appear in hospitalized patients
breakout more heavily in the summer
Most importantly, the epidemic itself had begun shortly after pharmaceutical companies received approval to manufacture the drug in Japan.
The End is near
On September 8 1970, the Japanese government banned all sales of Clioquinol.
In 1971 there were only 36 repaorted cases
In 1972, only 3.
In 1973, 1.
The epidemic was over.
In a conference in 1979, Reisaku Kono posed the question:
Why had research on the etiology of SMON not hit upon clioquinol until 1970?
Kono provided two answers.

Kono also observed that doctors refused to recognize the possibility of an iatrogenic cause. (Iatrogenic means it was caused by medical practice). The idea that the drug caused the symptoms it was being prescribed for in the first place - the cognitive dissonance must have been far too strong.
Furthermore, in the wake of the poliovirus campaign, the Japanese government simply had to keep up the momentum by funding the exact same institutions and people, but turn their attention to SMON.
The Final Throes
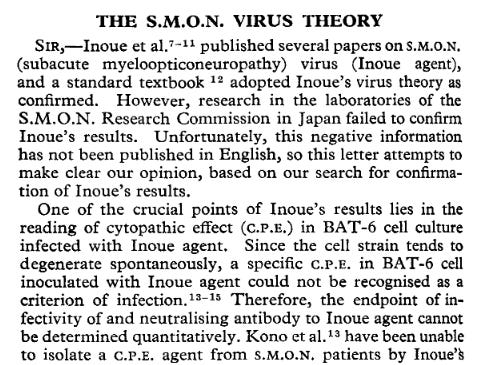
Despite these findings, it didn’t stop Professor Shigeyuki Inoue in Kyoto. With new claims of a fresh virus to put on the face of SMON, Inoue was published in several prominent medical journals, including The Lancet.

However, Inoue had his moment in the limelight and earned notoriety for discovering the “SMON virus". He even made it as far as mention in the textbook, Review of Medical Microbiology, 1974.
To Kono’s continued credit, he did not let these assertions go unchecked. He responded in a subsequent issue of The Lancet in August 23, 1975.
A string of legal battles ensued, and the controversy was resolved both within the SMON Research Commission and in court. Needless to say, there is no SMON virus. Even the US FDA had restricted clioquinol for 10 years before Japan.
Over the course of 15 years, over 11,000 Japanese people had become victim to the toxic effects of a drug.
Today, most people outside of Japan have never heard of the “viral” SMON epidemic. The story that SMON researchers had ignored the evidence of a toxic cause for 15 years, for a flawed viral hypothesis was too embarassing for establishment virologists to admit.
Credit Where Credit is Due.
I stumbled upon the above story in the first chapter of Peter Duesberg’s book Inventing the AIDS Virus. He shared this story as a backdrop, lesson, and prophecy of what had occurred in the US in 1980s - the AIDS epidemic.
For those of you who do not know who Peter Duesberg is, here is the only interview I can find of the infamous University of California, Berkeley Virologist by none other than Joe Rogan:
I have tremendous respect for scientists and doctors who pursue questions that the establishment actively censors.
The COVID pandemic has forced me to re-assess the integrity of the institutions that most doctors and researchers submit to, with little hesitation. In doing so, I have observed a pattern:
Respected scientists and Nobel Laureates are lost to infamy because they dared pose a question which opposed establishment narratives. Kary Mullis. Linus Pauling. Peter Duesberg.
The AIDS epidemic is one such narrative. It should come as no surprise that the same institutions and actors who have misled us during COVID, were the very same as those involved in the AIDS epidemic:
NIH/NIAID
Anthony Fauci
Department of Health & Human Services
Centers for Disease Control
World Health Organization
Great article. I’m motivated to study medical history even more now. I’ve been skimming the surface of medical history for the last several years & always interested to learn more. It seems there’s always more to the story. Be careful of appearances. And be wise to arrogance. Ugh: Semmelweis, the pediatricians in the 1960’s recommending formula over breast milk, the pediatricians in the 1990’s saying mothers should only breastfeed for 6 weeks, the food pyramid, statins, the current environment, etc.
Clioquinol was actually studied for treatment of alzheimer disease, long after the issues in Japan that are associated with it. There are all sorts of whacko alzheimer studies because of rich funding.
Clioquinol is processed more slowly and accumulates faster in humans than in various rodents that were studied. Middle aged women are likely to metabolize and eliminate many types of drugs more slowly than men and children, which might help to explain why they were hardest hit. Also absorption from the topical forms is pretty efficient, so those aren't a wonderful idea either.