

What Neurosurgery Got Wrong | Part 1
We have been taught for over a century that cerebrospinal fluid is made in the ventricles, and flows in a specific manner. But, is it made in the ventricles and does it even flow?

In all the years I have spent questioning the assumptions and information we take for granted within medicine, I never thought that we could have such a basic principle so wrong and due to such silly faults in our reasoning.
The mistake in our model of the nervous system that I am referring to relates to the nature and physiology of cerebrospinal fluid. To be fair, this is not merely a mistake of neurosurgery as a specialty - it is equally an error in basic anatomy and physiology, as it is an oversight for neuroradiology and neurology.
But, few disciplines make as much use of this model for both diagnosis and surgery as does neurosurgery.
For a week I have pondered how I would present this new information, and it seems to make the most sense to have this in two parts.
To really drive the point home and give you a sense of the magnitude of this error, in this first part I will discuss:
Basic neuroanatomy
What is taught regarding cerebrospinal fluid (CSF)
including how and where its made
where and how it flows
How we arrived at these beliefs about the CSF
Why its important for diagnosis and treatment.
What modern experiments and technology reveal about CSF.
I have not yet determined all the content that will follow in Part 2, but for starters we will embark on trying to understand diseases processes from the new model that follows from modern research.
Basic Neuroanatomy
To demonstrate how basic and foundational this physiologic mechanism is to get right, I need to go back to the basics.
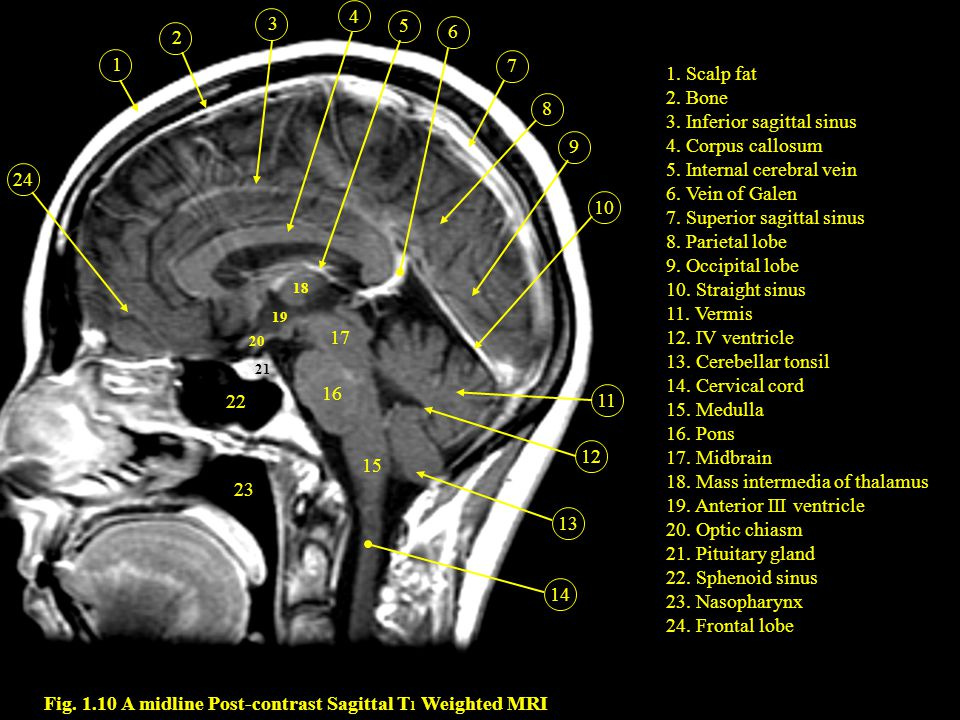
When I say basic, I mean knowing that there is brain matter, with very broad differentiations of the regions - cortex, basal ganglia, brainstem, & spinal cord. Because, the topic we are concerned about includes the ventricles, subarachnoid space, cisterns, dural sinuses, and their relationship to our cardiovascular system.

Inside the brain, there is a ventricular system which is continuous with the subarachnoid spaces. There are subarachnoid spaces surrounding the grey matter of the brain and cord. Around the cortex they are called sulci, around the brainstem they are called cisterns, and the cerebellar folds are called folia & fissures.
The dural sinuses are large channels of persistent venous flow. People (myself included) have a poor model in terms of understanding the true relationship of the dural sinuses. It’s not that the spaces of CSF drain directly into veins, which eventual drain into sinuses.
Although in some cases they may, this is probably not the general rule.
In reality, it may be that the CSF spaces around the brain have a capillary system of their own, and which varies in porousness depending on location of CSF production. Just like the veins draining brain matter eventually drain into the sinuses, so too would the veins of the meninges (the layers of covering that make up the sac which holds CSF).
Why?
Well, CSF is almost entirely water. Which means the effective volume of CSF will be determined by the location of highest blood-brain barrier water porosity. This, it appears, is greatest around the brainstem.

Why is the location of production important?
Good question.
Because, of our current understanding.
The Current Paradigm

We are taught that CSF is produced by a plexus (plica) of choroidal tissue (choroidea) inside the ventricles. The largest mass of which lives in the lateral ventricles. With a relatively small amount on the roof of the third and fourth ventricles.
But mostly, CSF starts in the lateral ventricles.
According to our model, not only does CSF demonstrate bulk flow, but it does so in a manner that starts in the lateral ventricles and flows down and out.
In the brain, that means traveling down the foramen of Monro into the third ventricle. Then, through the aqueduct of Sylvius into the fourth ventricle. Then out through the foramina of Luschka & Magendie into the basal cisterns and subarachnoid spaces surrounding the brain.

Along the spine we are taught that is flows down along the dorsal side (behind) of the cord, and up through the ventral side (in front)…even though there’s nothing really separating the ventral and dorsal side of the cord. It is one continuous space that the cord sits in.
You can see this most vividly on a lumbar spine MRI.

In both views, the bright white around the nerve roots in the spinal canal is CSF. That is how water looks on a T2-weighted MRI image. Notice the lack of any division of the chamber in front of the cord (to the left A or in front B) and behind the cord (to the right A or behind B).
But for some reason, we teach that there is bidirectional flow here.
More generally, we simply assumed that CSF flows…most likely because whenever we poke a hole in the CSF sac…fluid flows out. But the CSF space isn’t a channel like blood vessels.
Blood flows from point A to point B using arteries and veins. Waste & water due the same via lymphatic channels.
So must CSF, right?
Well, not exactly.
It isn’t that the CSF compartment is a channel moving fluid from one location to another. How do I know that?
Because when we are doing diagnostic testing of the CSF, it doesn’t really matter where you get it from. That’s why we often pick the safest location, hence the term lumbar puncture. We choose the lumbar region because there is no spinal cord (in most people) below L2. Thus, the CSF space is uniform.
Unless of course there is a physical obstruction - e.g. complete effacement of the CSF space due to a cord lesion. Then, it’s reasonable to suggest that there may be differences in fluid constitution above and below and obstructive lesion.

Because it doesn’t matter where you take a sample of CSF, favors the notion that CSF is a uniform space that the brain and cord are housed in. For example, the room you’re in right now has no reason to have the air inside of it flow…unless there’s some external force acting on it. An open window, air conditioning, or a fan.
If it is the case that CSF is a uniform diffuse space…why would it flow spontaneously, of its own accord? It wouldn’t. And, as has been recently demonstrated…it doesn’t.
Instead of bulk flow, what we actually see is pulsatile motion.
The best way to visualize this is to imagine you are in a large room shoulder to shoulder with people.

You are one of these water molecules. You resonate with and against one another. You aren’t moving from one location in the room to another.
That is for the objects which are dissolved in CSF (<1% of its composition).
When you put a single drop of dye in a container full of water, what happens?

The movement of the dye does not represent the movement of water. The water is still. It represents the rate of diffusion of the dye, or bumping into and along the water molecules. That’s why when it is cold, the leading edge of the dye moves down (with gravity) much more slowly. Low rate of vibration of the water molecules, results in lower rate of diffusing along them.
The problem? This is precisely how we have and continue to study the “dynamics” of CSF. For example, using radiotracers (a dye) dissolving along the CSF space. We use these low time-resolution projections of tracer location to infer motion.

Even at 24 hours, the tracer remains in the core ventricular cavities of the brain and to some extent, along the periphery. If CSF is flowing from the center of the brain (location of choroid within lateral ventricles), why would it still be there in greatest quantity at 24 hours?
In fact, why would it accumulate there at all, if the tracer is injected way down in the lumbar spine. If there is constant flow of CSF down from the center of the brain…how would the dye move back up there?
The answer is, it doesn’t flow. The tracer is diffusing down a concentration gradient, and then accumulating in the areas with the most static CSF - the lateral ventricles, and subarachnoid spaces past the Sylvian fissures.
Our current model claims the site of reabsorption of CSF are arachnoid granulations. Not centered around the brain. What most don’t know is that there are arachnoid granulations around the brain and along the length of the spine.
Thus, based on the model of constant flow…residual tracer should be seen last along the sites of reabsorption. Not in the center of the brain.

What Is Really Going On?
When I showed you the dye dissolving in water, I left out an important part.
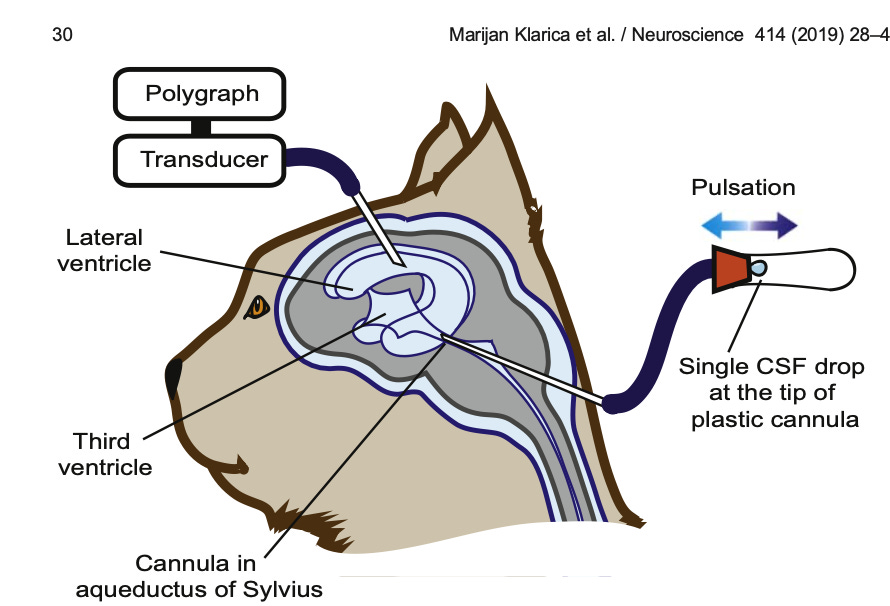
We have ample evidence which demonstrates that CSF does not flow. When we place a needle connected to a pressure normalized tube, and watch this 1 drop of CSF move back and forth for two hours, we have clinical evidence that CSF does not “flow” in bulk. It pulsates.
When we look at the motion of bands of water molecules in an MRI slice along the brain and spinal axis, we see that the water molecules vibrate, bump into each other and travel in both directions only a few millimeters before losing their momentum.

So in addition to vibrational motion and diffusion, there is also pulses of increased activity along the CSF space. Imagine you poke a puddle of water, and waves of water disperse outward for a few seconds before stopping. In fact, several studies have now shown that the there is no net motion of water within the CSF outside of the regions of CSF production and absorption into the bloodstream.
This finding is particularly damning when looking at the movement of CSF between the lateral and third ventricles. Time and time again, we find that there is no net flow between these chambers.
Of its own accord, CSF is mostly still. But when it is poked, it pulsates. This type of diffusive and pulsatile motion happens throughout the CSF space, with the exception of the lateral ventricles. Contrary to medical education, the CSF in the lateral ventricles barely pulsate. Rather paradoxically, the only real movement we can visualize is CSF moving into the lateral ventricles from the third.
Several researchers have now observed the opposite of the mainstream paradigm - that CSF water is moving from the third ventricle up into the lateral ventricles.

What causes the CSF to pulsate? Quite a lot.
Contractions of the heart, the expansion of the lungs, and the flow of blood impacts the pressure and tension along the membranes that form the sac of the CSF space (called the meninges).

When the heart contracts, CSF moves from top to bottom. When the heart relaxes, it moves from bottom up.
When you lie on your back, the cord and brainstem fall towards the back of their chamber, altering local movement of CSF.
The areas where exchange of water between the bloodstream and CSF space is highest, can be thought of as the boundaries along which CSF (water) is made and reabsorbed.
This video is a time-lapse of an MRI technique which has been optimized to detect the diffusion of water molecules of a certain location and speed. What you see in black demonstrates the local movement of CSF water molecules, and the intensity of the darkness demonstrates the degree of heterogenous (non-uniform) movement.
Contrary to what we are taught, there is virtually no motion of water in the lateral ventricles, where the modern paradigm claims CSF is made.
Further, the most motion of water exists along the surfaces surrounding the brainstem and third/fourth ventricles. Throughout several cardiac cycles, this region maintains its constant motion. This suggests that in addition to being the site of absorption of CSF water, it is likely also the location of filtration of new CSF water from the bloodstream.
This has also been demonstrated in animal models, whereby the animal was injected with a penicillin based tracer, and staining of the dye demonstrated where it was getting reabsorbed the most.

It wasn’t in the dural sinuses. It was along the surfaces of the brainstem, cerebellum and spinal cord.
What Does This All Mean?
For starters, many diseases of CSF that we diagnose and treat are based strongly on assumptions of where it is made, where it flows, and how it exits.
Whether this is the use of surgical devices to promote or limit the flow of CSF from one direction to another, to prescribing drugs, or in general understanding of the nature of disease - e.g. intracranial hypertension, intracranial hypotension, hydrocephalus, dementia, etc.
Beyond basic fluid dynamics, we need to reconsider when treating “obstructive” lesions of the ventricles. Location & nature of production as well as the rhythmic pulsatility of CSF around the brainstem suggests impact and function on neurological function that we had not previously considered.
For example, around the brainstem are several glandular organs which act as portals of communication between the endocrine (hormonal) system and the brain. These include the pineal and pituitary glands. The discovery that CSF is made in a location with the most fertile exchange of signals coming from the rest of the body, opens the door to a revolutionary way of thinking about brain function & disease.
Furthermore, if indeed the pulsations of the body reflect in pulsations along the brainstem, the implications are broad. Most of the brain matter in and around the brainstem control a wide number of physiologic functions, including:
Feeding
Emotion
Fear
Threat response
Balance & Posture
Cardiorespiratory function
Sexual drive
For example, what does it mean that we can modulate our basic nervous system functions with simple breathing exercises?
Is it only via top-down nervous system regulation?
Or does the shift in rhythm, rate, and amplitude of pulsation within the CSF have an effect on the basal rate and bias of neurologic processing along the brainstem?
We know that CSF is mostly water. We know that water acts as an information highway, and an integral part of energy storage and transfer.
Stay tuned for Part 2:
In his book "Longevity" Dr. Peter Attia asserts that we are moving from Medicine 2.0 (current) to Medicine 3.0 where study goes in much greater depth. At 76 I most likely won't see the ultimate outcome, but I suspect in another 30 years or so our current medical treatment will be regarded the same way we now regard the leeches for bloodletting. My dusty BA in mathematics leaves me with a limited grasp of biochemistry, but it's really interesting to see physics becoming equally important. Looking forward to part 2!
Deeply fascinating. (Or maybe fasciculating!) I've been helping the conventional notion by illustrating it in my courseware. If this is wrong, the animation needs to change.
http://ockhamsbungalow.com/FIPSE%20Audin/csf.gif