

International Grand Jury | Day 3: The PCR Test
An international grand jury investigating crimes against humanity has kicked off.

The Grand Jury - Day 3
For those of you who have no clue what this is about, check out this twitter thread for background info:

If you haven’t read what I learned from Day 2 - check it out here. Things got really meta when the man I wrote about, Alex Thomson, went on UK Column News, and discussed this very blog (starting at 43 minute timestamp).
Thank you for the kind words, Alex:
My parents were delighted to hear that.
Day 3 - The PCR Test
By now, you have probably heard from several sources about the unreliability of the PCR test used to diagnose COVID-19
First you heard it from your crazy friend, who seemed really conspiratorial
Then, you heard it from scientists online
Eventually, you heard it from the horse’s mouth: the Experts
During the third day of proceedings, several experts got together and discussed all the historical, technical, and practical implications of the PCR test. It’s all very nerdy & fascinating. Just the way I like it.
But, it has struck me over the years that no matter how meticulously you dissect the technical consideration of molecular testing and its role in a clinical diagnosis…people just don’t seem to be moved.
That’s not to say you shouldn’t listen to the testimony - you most certainly should.
What I am saying is that there is a much more fundamental way to understand the PCR problem.
What is the PCR problem?
In my opinion, the way that PCR has been leveraged in this pandemic is complete bullshit. It’s practically fraudulent - at the very least, intentionally deceptive.
But, what is the fraud, exactly?
Is it: PCR can be used to diagnose COVID-19?
No.
Is it: PCR can be used as a diagnostic test?
No.
I mean yes, both of those statements are false. But, no.
The fraud is this:
The disease was defined by a PCR result.
The PCR was the center of the pandemic case count from ground zero. PCR test-kits were hoarded before the first case of “COVID-19” was ever diagnosed. The PCR test designed specificaly to ‘diagnose’ COVID-19 was developed before we even knew there was an outbreak.
To understand what I mean by the statement “disease was defined by a PCR result,” we need ti look at the outcome matrix for COVID-19 testing:
Practically any symptom + PCR-positive → COVID-19
Flu-like symptoms + PCR-negative → Not COVID-19
No symptoms + PCR-negative → Not COVID-19
No symptoms + PCR-positive → Asymptomatic COVID-19?!
What is my point?
Apart from the claim I made above, I don’t have any other point.
If you accept the outcome matrix of our current testing paradigm, then you accept that disease is defined by the PCR test. Because, there is a 1:1 correspondence of test-postive to “disease.” Even in cases in which you have no symptoms, you are expected to behave and treated as if you are diseased.
Thus, I simply have questions for you to consider:
What is disease?
How do we diagnose disease?
How do we know if a microbe causes a disease?
How do we diagnose infectious disease?
What is the difference between a diagnostic and screening test?
Can a screening test be used to diagnose disease?!
What is disease?
Well, we can start with a definition of disease.
According to Merriam-Webster:

That’s not bad. A condition that impairs normal functioning and is manifested by signs and symptoms.
How about Wikipedia? Just in case we are being accused of cherry-picking:

Pretty consistent, wouldn’t you say?
You may be thinking that you know people who have a disease, but they are currently not showing any symptoms. That’s completely fair. In fact, depending on how you want to describe what it means to be ‘diseased,’ it is a totally viable argument.
The above contention is valid for chronic conditions which have been temporarily subdued by relief of symptoms - not the underlying problem. Because, if you addressed the underlying problem…well, you wouldn’t have chronic disease. You’d be cured. Here, you could argue that despite the symptoms being alleviated, the underlying disease is still present, and would rear its ugly head if you stopped treatment.
The whole point of making a diagnosis in view of symptoms (amongst other information) is to understand the underlying pathophysiology and address that. Not to mask the disease by solely alleviating symptoms.
Regardless, this article is to be discussed in the frame of infectious disease. These are illnesses caused by a microbe (e.g. bacteria or virus). Infectious diseases are often acute problems. But, even when they are chronic infections, they occur with symptoms. Otherwise, you would not know to look for a microbe in the first place.
“But what about dormant or asymptomatic infections?!”

Time for our first detour.
Despite what your eyes may be telling you, there are microbes literally everywhere all the time. Around you, on you, and inside you. Gazillions of them. Just because you decide to look for one microbe, at the exclusions of millions of others, does not mean it is the causative agent of a disease.
For great examples of this in practice, and rather comedic examples of medical history, check out these prior pieces on Scurvy, Pellagra, and the 15-year epidemic in Japan that never was…
There are countless bacteria, viruses, and fungi present on our person at any given time. Some help us, some hurt us. Those that hurt us will encounter our immune system.
Through an intricate dance, our immune system will develop an understanding of the microbe and strike a balance. The microbe can hang out, just as long as it doesn’t multiply to an extent that it can cause pathology.
Our immune system is an incredible work of evolution. But, if anything were to weaken our immunity, those microbes that were previously under control could multiply and cause illness.
Fundamentally, if a microbe is present and there is no indication of illness (ie. asymptomatic), then it is harmless - at least under the current condition of the host’s immune system.
Without indicators of illness, you cannot claim there is disease - as such.
How do we diagnose disease?
Next, we must explore what a medical diagnosis actually is.
Again, we can refer to Wikipedia here:

We can definitely work with this definition.
Diagnosis is a process of determining which disease or condition explains a person’s signs & symptoms.
Sometimes patients might not have any signs or symptoms - maybe just a blood test with a result outside the normal range. For the purist, to assume that a test result is sufficient to diagnose a state of illness in the absence of all other factors, is also questionable.
Good example: you try a ketogenic diet, or start intermittent fasting. You are losing weight, eating healthy and feeling great!
But, then you doctor performs the annual tests and discovers your cholesterol is above the normally accepted range. Are you ill? Is this a disease?
One of the my favorite mentors would drive this point home:
Treat the patient, not the numbers.
What is infectious disease?
To be able to diagnose an infection, we first need to establish a causal relationship between the microbe and illness.
For that, we need to take another detour.
Koch’s Postulates are four criteria designed to establish a causative relationship between a microbe and a disease.
Koch’s first postulate states:
The microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms.
This is a two part statement.
First, the microorganism must be found in abundance in all organisms suffering from disease.
Not only must the organism be found
But, it must be found in abundance - keep this in mind, for later
Secondly, it should not be found in those that are healthy - AKA asymptomatic.
The idea that you can suffer from an infectious disease without symptoms is void by the first criterion we use to establish a relationship between microbe and disease. Because if there are no symptoms, and no disease - there is no illness.
Koch’s second postulate states:
The microorganism must be isolated from a diseased organism and grown in pure culture.
The microorganism must be isolated and grown in pure culture.
Viral culture is not used to diagnose COVID-19. Do you know anyone that got their sample cultured? Neither do I.
Viral cultures are more often used for research purposes. But, even then viral culture is rarely positive after 5 days of symptom onset. Which means that the pictures and videos of ICU patients are people who are culture negative - almost all of them. Thus, whatever is going on with their body and immune system at the time, is not a function of an acute viral infection. More than likely, it is due to either an immune/inflammatory state, a hospital-acquired infection, or a complication.
Koch’s third postulate states:
The cultured microorganism should cause disease when introduced into a healthy organism.
Well, other than spending time with people who are test-positive, we don’t actively introduce cultured SARS-CoV-2 into healthy people…at least not voluntarily.
The positive test defines presence of microbe in the case of SARS-CoV-2. And, if people can be asymptomatic (aka without disease) with the microbe, then it is the case that some people are not diseased when the microbe is introduced into them.
Koch’s fourth postulate states:
The microorganism must be reisolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent.
For all intents and purposes, this is not done. Actually, I don’t think this has ever been done. Correct me if I’m wrong, please.
So, how do we diagnose an infection?
Well, there are a few ways we can diagnose disease.
One way is to analyze the patient’s medical history, physical examination, and chief complaint. Using our medical knowledge, we try to come to a diagnosis without additional testing.
With respect to infections, this form of diagnosis is termed pathognomonic.
Pathognomonic (rare synonym pathognomic[1]) is a term, often used in medicine, that means "characteristic for a particular disease". A pathognomonic sign is a particular sign whose presence means that a particular disease is present beyond any doubt..
The problem with COVID-19 pneumonia (a respiratory tract infection), and indeed any seasonal respiratory infection, is that their symptoms have exceptional overlap. There is no way to single out a specific virus on the basis of symptoms alone.
Another way to diagnose a disease, is to test for it.
With respect to infections, there are several categories of tests:
Microscopy - simply look for the microbe under magnification
Culture - provide an environment in which a targeted microbe can flourish
Biochemistry - include the detection of metabolic or enzymatic products characteristic of a particular infectious agent
Molecular Testing - Serological, Rapid antigen, PCR, genomic sequencing
For logistical and historical reasons, several viral infections are “diagnosed” by molecular testing. There are numerous problems with molecular tests used in the clinical setting. With respect to pneumonia, molecular testing is not needed, and treatment is usually successful without knowing the causative pathogen.
Culture is the gold-standard for the diagnosis of many infectious diseases, but particularly for bacteria. Culturing virus is also important. If there is no viable viral sample present, then there can be no infection.
The whole point of an acute infection is that a microbe evades immunity sufficiently to allow for rapid multiplication and spread. This increased infectious mass and proportional immune response can be overwhelming to the host.
If you cannot extract viable viral sample, then it’s likely not the cause.
The problem is that viruses are notoriously difficult to culture.
Some might consider competing hypotheses to account for this:
The virus in question is not the actual cause of the observed disease. It is so well controlled by the immune system, or it is absent to the extent that successfully culturing the porposed virus has proven difficult.
Our lack of understanding of viruses is so profound that we have difficulty either:
Creating the environment that would foster the growth of this virus.
Our hypothesis is incorrect about the causal relationship of this microbe and the observed illness
Brass Tacks
We cannot isolate an abundance of virus in all people suffering from the disease.
And we do diagnose presence of virus in perfectly healthy people (asymptomatic cases)
Koch’s First Postulate: Failed.
Because we could not isolate viable virus (SARS-CoV-2) from nearly all of the cases which were admitted to the hospital, we turned to molecular testing.
It probably went something like this:
Ok, we cannot get live virus.
What if we check for a gene fragment that we believe to be representative of the SARS-CoV-2 virus?
This is where we enter the world of Polymerase Chain Reactions. In brief, this lab test takes a sample, and breaks down all the living tissue to expose DNA fragments. After, you add a fluorescent tag for your target sequences (which is a mere fraction of all of the sequences that could be tested for in any given sample), and start performing cycles of amplification. Then look for whichever tagged sequences produce visible light first or strongest (due to exponentially increasing quantity with each amplification cycle).
From this result: a gene fragment present in sufficient quantity to produce light when amplified…
We somehow arrive at: you have been infected with SARS-CoV-2 regardless of all other factors.
You have flu-like symptoms? COVID-19.
Gastrointestinal symptoms? COVID-19.
Headache? COVID-19.
Stroke? COVID-19.
No symptoms? No problem! Asymptomatic COVID-19.
Do you see where I’m going with this?
It’s a categorization game. It has nothing to do with disease. It has nothing to do with identifying the causative agent.
You will not feel safe or breathe easy unless you test yourself for…COVID-19.
Is this even a diagnostic test?
No.
It is not.
PCR and Rapid Antigen tests are screening tests.
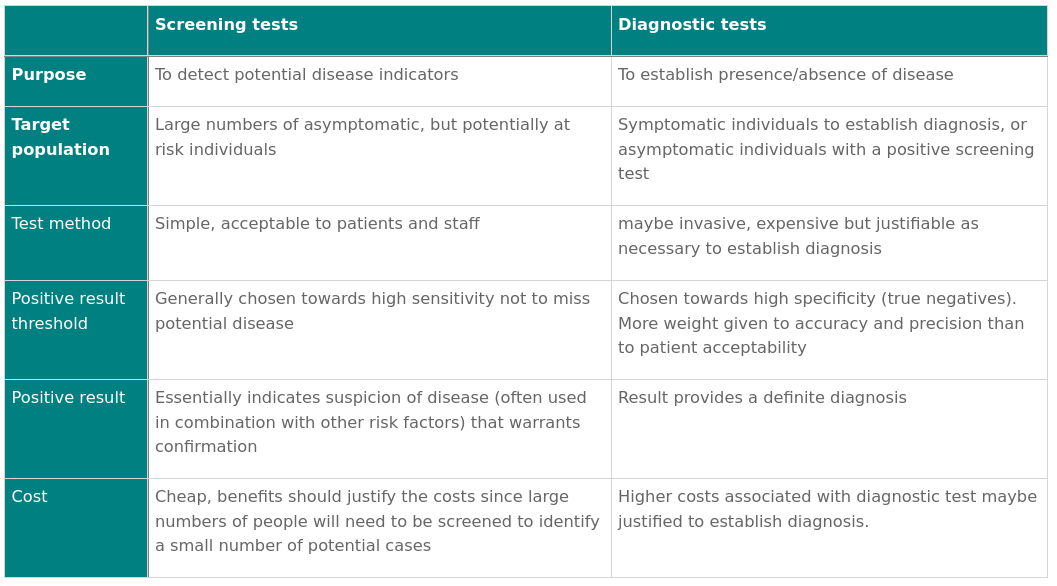
Screening tests, as you can see, are not diagnostic tests.
They do not establish causality. Why are they not diagnostic? Because, they do not meet the standars set by confirmatory testing, such as live culture.
Koch’s Second Postulate: Failed.
Remember, viruses are all over us, all the time. Even in places we did not previously believe them to be - like the lungs. Yes, it turns out there are viruses present in our lungs and cause no illness - AKA asymptomatic.
Day 3 of Grand Jury Testimony
The first witness, Dr. Astrid Stuckelberger made an astute observation from the outset. In comparison to SARS-CoV-1 (2002 SARS Outbreak), during the SARS-CoV-2 epidemic the PCR test replaced the doctor.
During CoV-1, the diagnosis and management of these patients involved the doctor. Doctors were at the center of the validation process.
This practice, for whatever reason, disappeared with SARS-CoV-2.
Dr. Stuckelberger identifies several problems, many of which reflect on the problems of causality outlined above.
Ponder this Problem
Now that we’ve set the foundation.
I ask again: What is the fraud, exactly?
Is it: PCR can be used to diagnose COVID-19?
No. We were misled here.
Is it: PCR can be used as a diagnostic test?
No. By its very nature, PCR cannot be diagnostic. We were misled here, as well.
The fraud is this:
The disease was defined by a PCR result.
To appreciate just how meaningless this application of PCR technology is, we need only look at the outcome matrix for COVID-19 testing:
Practically any symptom + PCR-positive → COVID-19
Flu-like symptoms + PCR-negative → Not COVID-19
No symptoms + PCR-negative → Not COVID-19
No symptoms + PCR-positive → Asymptomatic COVID-19?!
Alas, if you don’t find the above rhetoric very convincing, then you could always listen to the experts discuss all the technicalities.
Day 4 of Grand Jury proceedings are today, February 19th.
The arrogance of man knows no bounds. The potential damage is likewise unlimited.
Follow me on Twitter @RemnantMD and Instagram @remnant.md