

How to Make a Pandemic.

Introduction
Since the declaration of a Public Health Emergency of International Concern (PHEIC), the population has been under the impression that their world has been turned upside-down and inside-out by a globally concerted effort to mitigate the damage from a seasonal respiratory virus.
At least, that is the story.
For those attentive few who did not buy into the global marketing campaign, it would appear that the last two years has been one damning revelation after the next.
It’s been quite the hunting season for conspiracy theorists.
Outstanding Questions
I thought it would be appropriate to take stock of what we were told has happened, and compare it to what has actually happened…in an attempt to navigate a future that is approaching much faster than even the most cynical amongst us had expected.
I fear that in an attempt to resolve the cognitive dissonance, our collective conscience has decided that everything we have done was worth it…which may - nay, will be used as justification to do it again…
History has taught us that even experts & doctors are susceptible to this sort of cognitive frailty:

So, then…
Where & when did SARS-CoV-2 come from?
Was our response effective, or even appropriate?
Where did the Influenza go?
Did our actions result in net harm?
What was it all for?
From the top…
On January 22, 2020, the WHO convened its first emergency meeting…and determined that there were not enough cases, nor sufficient international spread to declare a PHEIC.
Just 8 days later…both requirements were miraculously met!
What changed? Briefly, from the above article…
Christian Drosten of La Charité Berlin, in collaboration with Olfert Landt at TIB MolBiol (biotech company), already had the documentation for a completed PCR-test kit for ‘novel’ coronavirus-2019 on January 15th.
This test kit was ultimately purchased and distributed by Roche.
The completed Drosten PCR protocol (45 cycles) was submitted to the WHO.
The WHO disseminated the Drosten protocol to the member States.
The member states bought the test kit from Roche, and deployed it onto their population.
And, as dictated by the International Health Regulations (WHO Constitution), any test result that came back positive was submitted to the WHO.
Then, upon convening on January 30th, the WHO were able to confirm increased cases of this novel pathogen across multiple jurisdictions.
But…
How do we know that SARS-CoV-2 was not in circulation before the availability of the first test?
I mean…just because we couldn’t detect this virus, does not mean it was not in circulation. This should be painfully obvious to even the most stubborn Covidian.
The real question is…just how long has ‘CoV-2’ been in circulation. Because, if it’s been in circulation for years…then what were we trying to mitigate, exactly?
For example, the Wuhan Military games were held in October 2019.
Or, how about March 2019?

If you recall, in 2020 we were told to put our lives on hold for 2 weeks to mitigate the rapid spread of a seasonal respiratory virus.
Do you think that almost a full year and an entire flu season (2019-2020) would have given SARS-CoV-2 enough time to circumnavigate the globe? Before we had even declared a PHEIC?
I’m not a biologist…but, yes.
A Twisted Timeline
Ok, so it turns out SARS-CoV-2 was in circulation long before January 2020.
You may even think:
March 2019 is not that far behind 2020…right? This is all still kosher…
Well, then how about this?

In 2016, Stephane Bancel (CEO of Moderna) et al filed the patent application above.
Modified polynucleotides for the production of oncology-related proteins and peptides
Translation: gene sequence for cancer-related protein.
Here’s where things get weird again…
SARS-CoV-2 genome is most similar to RaTG13 bat coronavirus (96.2%)
The key difference is 12-nucleotides in the Spike protein encoding the amino acids PRRA
PRRA is within the Furin Cleavage Site - an artificial sequence responsible for enhanced pathogeneticity, and the synthetic component of SARS-CoV-2
Punch line: The 12-base sequence in the virus is a 100% complementary match to the sequence (SEQ ID11652) in the above patent.
You can read more on this below:
The point is this:
SARS-CoV-2 Spike protein contains an artificial sequence which is a 100% match to a patented technology from 2016, which encodes a human DNA mismatch repair protein.
The Disappearing Flu
Readers will be familiar with the phenomenon of missing Influenza during the 2020-2021 season.
At a Level 1 Trauma Center in a major hospital network on the East Coast, the standard protocol for admission includes testing every patient for SARS-CoV-2 using a multiplex assay from Roche, which advertises the ability to test for SARS-CoV-2, Influenza A & B in one-stop shop manner. This is called a multiplex assay.
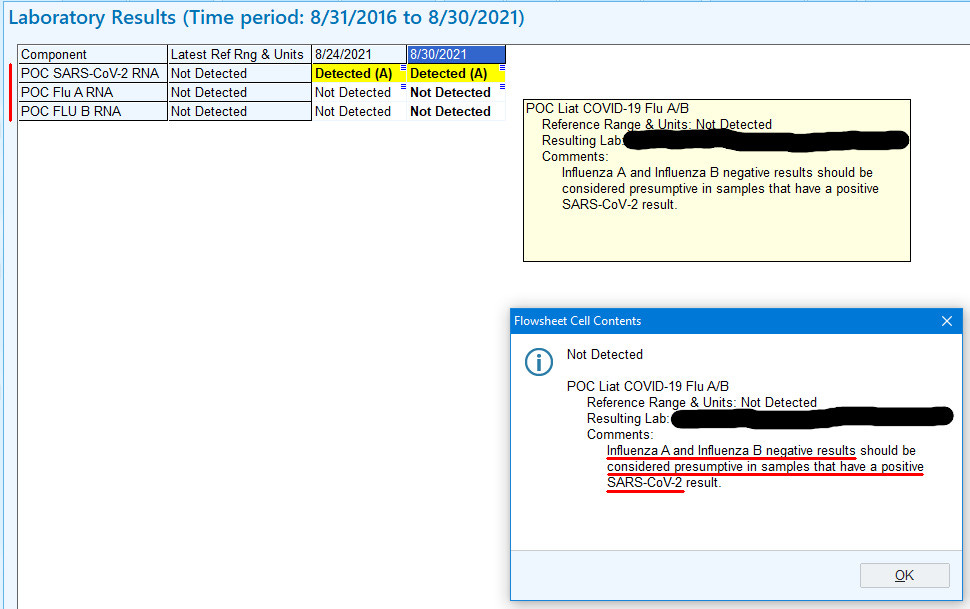
Notice anything interesting on this test result?
Take a closer look…
In English: if a sample tests positive for SARS-CoV-2, it is presumed to be negative for Influenza.
But, why? Page 24 of the documentation for the test…
studies showed that SARS-CoV-2 virus...can inhibit the detection and amplification of influenza A and influenza B virus RNA...and may lead to false negative influenza virus results
“Studies showed”
Surely, there must be a reference to back up this claim. Or even some data from their own testing. Alas, there is nothing in the documentation to back this up.
The use of PCR testing for diagnosis of SARS-CoV-2 was riddled with problems from the onset:
In addition to the unreliability of PCR to diagnose COVID-19, we also have the added problem of it effectively wiping out the detection & counting of Influenza.
Here is a simple scenario:
Hospital needs tests to screen patients for COVID-19
Roche & competitors offer a multiplex assay which tests for COVID-19 and Influenza - what a bargain!
That test by default will exclude the possibility of diagnosing Influenza, if indeed it tests positive for COVID-19
Surely, there was some benefit…
When you consider everything that was done to us, our loved ones, our businesses, livelihoods, constitutional rights - our children!
What was all that for?
Certainly not for nothing…right?
Well…I guess it depends on your definition of ‘nothing.’
Don’t take my word for it, that 0.2% comes from a Johns Hopkins study.
What was this all for?
I firmly believe that most of what is happening is not out of overwhelming concern for the health and well-being of the population at large.
Since when has any contemporary government gone to such lengths for your health?
So, what was it for?
The writing is on the wall, my friends. You need only look.






The actual risk from the virus was not discussed. By the summer of 2020, even a non scientist like myself could determine that people under 60 were largely unaffected. But you had to look for this information. Instead we got a hysteria over “cases,” which for the first time included people who weren’t actually ill. Instead we got mask mandates. Masks were very effective at spreading fear in the absence of information about the true risk. The widespread testing should have shown that the vast majority recovered, but instead the ratio of positives to deaths wasn’t mentioned. The hospital and death numbers were both hyped to the skies by counting every illness and death in the covid tally, even if the person had been admitted for another reason, like terminal cancer. Finally any medical professional who spoke out was demonized. Let’s not forget this disgraceful episode.
Doc, this is such an outstanding piece of work. Thank you.