

First Principles | The Problem with Gene-based Injections - Part 1
The cellular environment is incredibly complex and dynamic. To understand the concerns with gene-based injections, we need to go back to basics.

Brief Background
Since the beginning of vaccine rollout, many people looked at me quizzically when informed that I had no intention of getting an injection of an experimental gene-therapy.
In their minds, these are vaccines. Furthermore, they are “Safe & Effective” according to the promos.
To me, there were far too many unknowns about the ‘vaccines.’ Conversely, by the end of 2020 we knew enough about SARS-CoV-2 that I had no concerns about catching it - if I hadn’t already.
By this time, I had a solid idea of whom I could not trust:
NIH & NIAID
CDC
FDA
Anthony Fauci
If I had any chance of making an informed decision, I had to incorporate the following:
Vaccine clinical trials
Including the methods, results, and supplementary material
Background knowledge of: immunology, cell & molecular biology, physiology, & infectious disease
Actual experts in a given field - not just Big Tech & Corporate News personalities
History - how have regulators & institutions handled other similar situations?
I am not saying that my approach was fool-proof. But, as time has revealed…it was a sufficient framework to protect my loved ones. Furthermore, the predictive capacity of the framework has paid dividends already.
The Ideology
Before we begin this exploration, let us give the devil its due.
For the archetypal ‘explanation’ of how the mRNA vaccines work, we can refer to the marketing material of Big Pharma.
A snippet from Big Pharma’s most well-known marketing firm, the CDC:
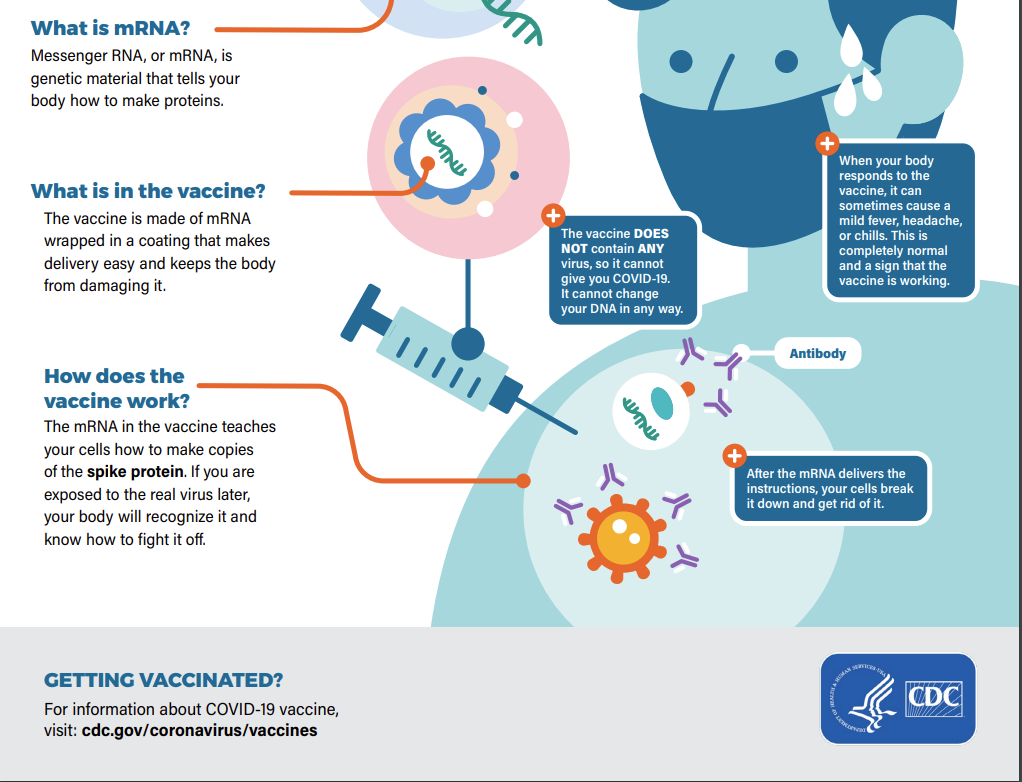
Based on the promotional material, it is all really simple:
We inject mRNA coated in protective material
Your cells take up the mRNA
produce Spike protein
Destroy the mRNA
Then your body generates antibodies against Spike
Simple. Safe. Effective.
Or is it?
The Conceptual Framework
We will be discussing various lines of biologic reasoning, so it would be helpful to keep these questions in mind as we progress through this endeavor.
What is dangerous about SARS-CoV-2?
How does adaptive immunity work?
How do these vaccines actually work?
What is autoimmunity?
How does the intersection of adaptive immunity and these vaccines affect the health of your body?
What evidence is there that this interaction is harmful?
What is dangerous about SARS-CoV-2?
Answer: Spike protein
Coronaviruses are ubiquitous. They have been with us forever. We have evolved together, to live in harmony.
People can get a cold from coronaviruses. Usually, this is due to an imbalance between viral load and immune status. Diminished immunity to the extent that a pathogen can no longer be kept in check is responsible for the symptomatic manifestation of several infectious agents - including coronaviruses.
Since coronaviruses have to contend with the immune system of countless organisms, including humans, they have a tendency to mutate. This characteristic makes them very poor targets for vaccination - as prior efforts have proven.
By the time a vaccine is developed and distributed for a given strain, the target coronavirus has already mutated
What was the solution to this?
A vaccine based on Spike protein - and only Spike protein.
A single-antigen vaccination strategy.
As if that were not enough, the antigen they chose is a surface protein with a high propensity to mutate. To understand why this is a poor strategy to prevent transmission of a virus, this article explains it rather thoroughly.
Spike protein is the pathologic component of SARS-CoV-2
This isn’t even a topic of debate.
Not only do corporate media ‘experts’ know that Spike protein is pathologic, but this has been known for decades. The idea that Pharma only learned about its toxicity after making the vaccine is absurd.
Coronaviruses and Spike protein have been studied for decades. Chimeric Spike protein was developed in labs years ago. The research, grant, and patent trail is undeniable.
We haven’t even gotten to the real problem.
The Spike protein on SARS-CoV-2 is not wild-type. It is a man-made chimeric Spike protein, that has been developed for increased pathogenecity. Chimeric Spike protein was developed as a bioweapon.
What did we do about that?
We took the genetic code for chimeric Spike protein, put it into a lipid nanoparticle and called it a vaccine.
Safe. Effective.
What is Adaptive Immunity?
The immune system compromises of innate and adaptive immunity.
Innate Immunity:
Innate immunity involves inflammatory cascades and recruitment of cells which consume and destroy antigens recognized as foreign.
Adaptive Immunity:

Adaptive immunity is a complex mechanism that serves two primary functions. First, it can function downstream to innate immunity to develop memory against the invader. Second, the memory can be activated in the presence of re-infection with the same invader - a rapid and devastating immune response. This is why natural immunity is so robust.
Adaptive immunity has two separate cell lines which serve specific functions: Humoral (B-cell) and Cellular (T-cell) immunity.

As illustrated above, T-cell immunity is usually discussed in the framework of CD4+ and CD8+ T-cells. The classical teaching is that CD4+ are helper T cells, and as their name suggests, they help the immune system recognize and recruit an army to handle the pathogen. CD4+ cells interact with antigen-presenting cells (APCs) through MHC Class II. This class of receptor is found on professional APCs: dendritic cells, phagocytes, endothelial cells, and B cells.

Alternatively, CD8+ T-cells (killer T cells) are involved in the destruction of host cells that are infected with a pathogen. Additionally, they are involved in the destruction of damaged and even cancerous cells. Pretty important. CD8+ cells interact with APCs through MHC Class I. This class of receptor is found on all cells that have a nucleus, and platelets. The interaction between the killer T cell and the APC generates a mature killer T cell, which can now recognize the antigen in question and kill infected cells.

I don’t mean to reduce the complexity of our adaptive immunity to just these two concepts, but this is adequate to continue our discussion.
Take home point: Cells which are infected with a foreign agent present the antigen on its surface so that CD8+ T-cells can:
Mature into killer T cells that recognize the antigen
Circulate around the body
Look for any cell (or platelet) which has been infected with this antigen
Destroy those cells
How do these vaccines actually work?
This is where things start to get a little concerning…
Here is a snippet from a Nature article entitled “mRNA vaccines — a new era in vaccinology”

Now, let’s clarify the steps involved in this Spike protein gene-based vaccination:
Spike-protein encoding genes are wrapped in lipid nanoparticles (LNP)
LNPs are injected into a human
LNPs then fuse with local cells, and also enter the bloodstream
The bloodstream spreads LNPs throughout the body
LNPs release the Spike-protein gene into the cell’s cytoplasm
The cell uses its machinery to make Spike protein - the antigen
Cells then present the antigen via MHC I → Train killer T-cells
Killer T-cells circulate around the body and destroy any cell that is presenting the Spike protein
This is the critical final step:
Before your cells fused with LNPs, they were healthy
After vaccination, killer T-cells now perceive those healthy cells as infected - requiring destruction
This is the definition of an autoimmune response - the host immune system turns on its own healthy cells.
Implications
The above is probably a lot to take in.
It implies that the global population is being injected with a drug that can generate an autoimmune response against any cell in the body. Some people will develop more severe complications than others.
It is consistent with the observation that those who suffer the worst complications from the injection, tend to be young & healthy - AKA with healthy & robust immune systems.
Strong immune system → Strong autoimmune response
These are serious implications. Do we have evidence to suggest this is happening?
Yes we do. In fact, we have two lines of evidence.
On the one hand there is population-level data that is sufficiently alarming to influence international vaccination strategies:
Rates of complications such as thrombosis, myocarditis, pericarditis, strokes and other end-organ damage are high in some demographics
High enough that some countries have not vaccinated children, and in some cases have forbidden the use of some of these vaccines in other subpopulations
At this point, most are aware of the population-level data.
What about individual-level data?
This has been far more difficult to come across. Many sources report difficulty in obtaining approval to autopsy people who have died shortly after vaccination - mere formality, I’m sure.
Some determined Pathologists, however, have been successful. Specifically, a German pathologist named Arne Burkhardt.

Burkhardt and his team have been performing autopsies and biopsies on people who have died or suffered complications after vaccination. He presented his findings on Day 4 of the International Grand Jury.
He showed two separate types of histologic stains.
One was a stain that was specific for Spike protein expression:

The above slide demonstrates a stain of vasculature positive for Spike protein (dark/brown staining inside the vessels) in the endothelium.
The second type of stain (H&E) demonstrated the presences of immune cells, specifically lymphocytes (T & B-cells are lymphocytes).

The above is from a person whose aorta ruptured - the aorta is the biggest & strongest artery in the body. If you look closely, you can see among the sea of pink (vessel wall) tiny dark blue cells - these are lymphocytes.
Why are there lymphocytes inside the walls of the aorta? Well…

…looks like they are in response to native cells expressing Spike protein.
What about myocarditis?

Above is another patient, this one with myocarditis, demonstrating invasion with lymphocytes - acute lymphocytic myocarditis. This eventually leads to…

…necrosis of the heart muscles (big white gaps between cells).
What about the brain? More Spike protein.

I think you get the point.
Believe me, this was not an easy realization to digest. I’m still blown-away that this is actually happening.
But, as attention is being shifted away from COVID to other geopolitical tensions, we must remain vigilant.
If these injections are causing short-term complications by a severe immune-mediated response…then what are the long-term complications? Easy to imagine in the case of myocarditis…
Myocarditis → Chronic scarring → Arrythmia → Stroke or Heart attack
What about long-term complications of the immune system?
Lymphoma?
Immune deficiency syndromes?
And the brain?
Disability from stroke?
Neurodegenerative changes?
The above, and more, have already been reported in the literature.
The long-term consequences are unknown & uncertain.
Be sure to check out Part 2: The Trojan Horse

The arrogance of man knows no bounds. The potential damage is likewise unlimited.
Paid subscribers enjoy:
Easy to understand perspectives on common health concerns
Research summaries relevant to your health
Insights from real case studies
Free Insights Preview:
Thank you for this article! It's both thorough *and* clear for the (mildly informed) layman.
If your expertise allows, would you be able to write another article about the implications of the recent discovery that the RNA from the Pfizer BioNTech shot can reverse-transcribe into human cells? The results of the in vitro study are here: https://www.mdpi.com/1467-3045/44/3/73/htm
This is fascinating and terrifying, but it's my understanding that researchers have known for a long time that reverse transcription was possible. It's just stunning what the medical and public health establishment has done to us.
Superb