

Can Statins Cause Heart Attacks?!
Statins are one of the most lucrative and widely used drugs to lower cholesterol. In recent years, more of its problems are coming to light.

Metabolic Machinery
It is no secret that I am not a fan of statins.
In fact, I am generally opposed to artificially suppressing cholesterol. Not least because cholesterol is one of the most important molecules in all of mammalian physiology.
Cholesterol is involved with:
Cell structure, fluidity and repair
Signaling, proliferation, migration and trafficking
Hormone production and balance
The list goes on.
Although you can continue to argue about the merits of lowering cholesterol for some survival benefit, there is no cholesterol therapeutic approach as harmful as statins.
If you are like most people (including doctors), you may think that statins simply lower cholesterol. This could not be further from the truth.
Statins (or HMG-CoA Reductase inhibitors) block an enzyme upstream to some of the most important functions of the cell. You can see from the diagram below that HMG-CoA Reductase is responsible for the production of all sorts of different molecules, in addition to all of the molecules derived from sterols (which are in the thousands).

One of the most well known molecules that statins deplete is Coenzyme-Q10 or Ubiquinone.
CoQ is an anti-oxidative protein that is part of the electron transport chain in our mitochondria. Mitochondria are responsible for making energy, and they does so by a process called oxidative phosphorylation facilitated by this transport chain.

Statins also block the production of Heme A. Heme A is a functional component of cytochrome c oxidase (Complex 4 in the electron transport chain).
Cells rely on mitochondria’s ability to generate ATP (energy) in order to survive & thrive.
Thus, anything which impairs optimal function of mitochondria will lead to cell dysfunction. As you can see, statins heavily inhibit the optimal function of our mitochondria.
Cells of the heart (cardiomyocytes) contain more mitochondria than any other organ in the human body. Which makes sense - the heart has a hard task, and it’s working nonstop.
From this information alone, it is completely reasonable to assume that any substance which interferes with energy production in this manner, will ultimately result in organ dysfunction.
Troponin & Heart
It would appear that some researchers share my concerns, and put this hypothesis to the test.
Now, the content of this experiment centers around changes in serum troponin levels.
Troponins are proteins which are integral to the normal function of muscle. In cardiology, we measure serum (blood) troponin levels in the diagnosis of heart attacks or other causes of damage to heart muscle.
The premise is that as heart muscle gets damaged (either by inflammation or ischemia), the cell leaks troponins into the bloodstream. Once we detect it, we become suspicious of heart damage.
There are different types of Troponins, measured by different tests. One of the more common tests is high sensitivity Troponin T (hsTnT). This is the troponin assay that was used in the study.
hsTNT is diagnostic of myocardial infarction (heart attack) when 22 ng/L in men, and 14 ng/L in women.
Additional data supports that in the healthy general population, levels 6 ng/L confers increased risk of cardiovascular disease/dysfunction.
Study Design
The authors recruited 56 patients without history of coronary artery disease, cardiac pathology or recent admission related to acute chest pain.
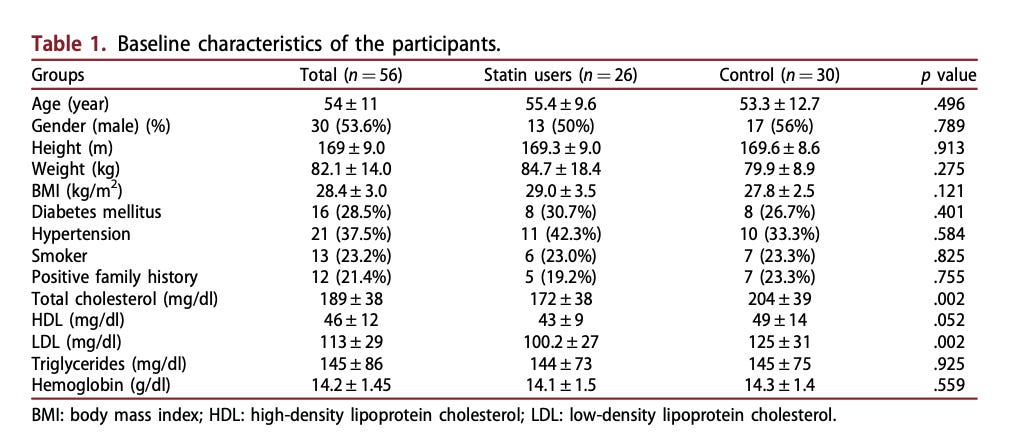
Information to note about this cohort:
Baseline characteristics were rather well balanced between the two groups including similar rates of: diabetes, hypertension, smoking status, and family history
The only difference (statistically significant) was the total cholesterol and LDL, which was lower in the group that was on statins (as we’d expect).
Both groups underwent moderate intensity exercise, which consists of 5 mins of treadmill at 2.5 km/hour (brisk walk), followed by 30 minutes at 5.5 km/hour (jog). Serum troponin was measured before and 4 hours after exercise.
Results

As you can see, the Statin users demonstrated a significant increase in hsTNT after exercise. Let’s review the numbers:
Average hsTNT after exercise in control group was 7.74 ng/L, highest of 13.5 ng/L, and an average increase of about 7.1%
Average hsTNT after exercise in the statin group was 11.4 ng/L, highest of 26.6 ng/L, and an average increase of about 43.8%
When comparing to reference ranges of hsTNT, you can see that some participants in the statin group demonstrate a level that is compatible with a heart attack (>22 ng/L).
The authors then applied a rule-out limit, which involves repeating the hsTNT after an hour to see if it is still high or returns back to baseline. When applying this rule, they found that 38% of statins users had consistently elevated hsTNT sufficiently high to suggest ischemia to the heart. Fundamentally, an indicator of damage to heart muscles. In the control group, only 10% demonstrated a similar increase (p=0.024).
What Does This Mean?
As we established, statins interrupt the mitochondrial and cellular machinery needed to properly generate energy & function.
When you exercise, you place an elevated metabolic demand (or stress) on your cells and organs.
But, if there is a discrepancy between the stress load (in this case, moderate exercise) and capacity to meet this demand…we begin to experience cellular dysfunction.
We typically think of a heart attack as a scenario in which there is not enough oxygen getting to the heart, usually because of a blockage of the coronary arteries.
